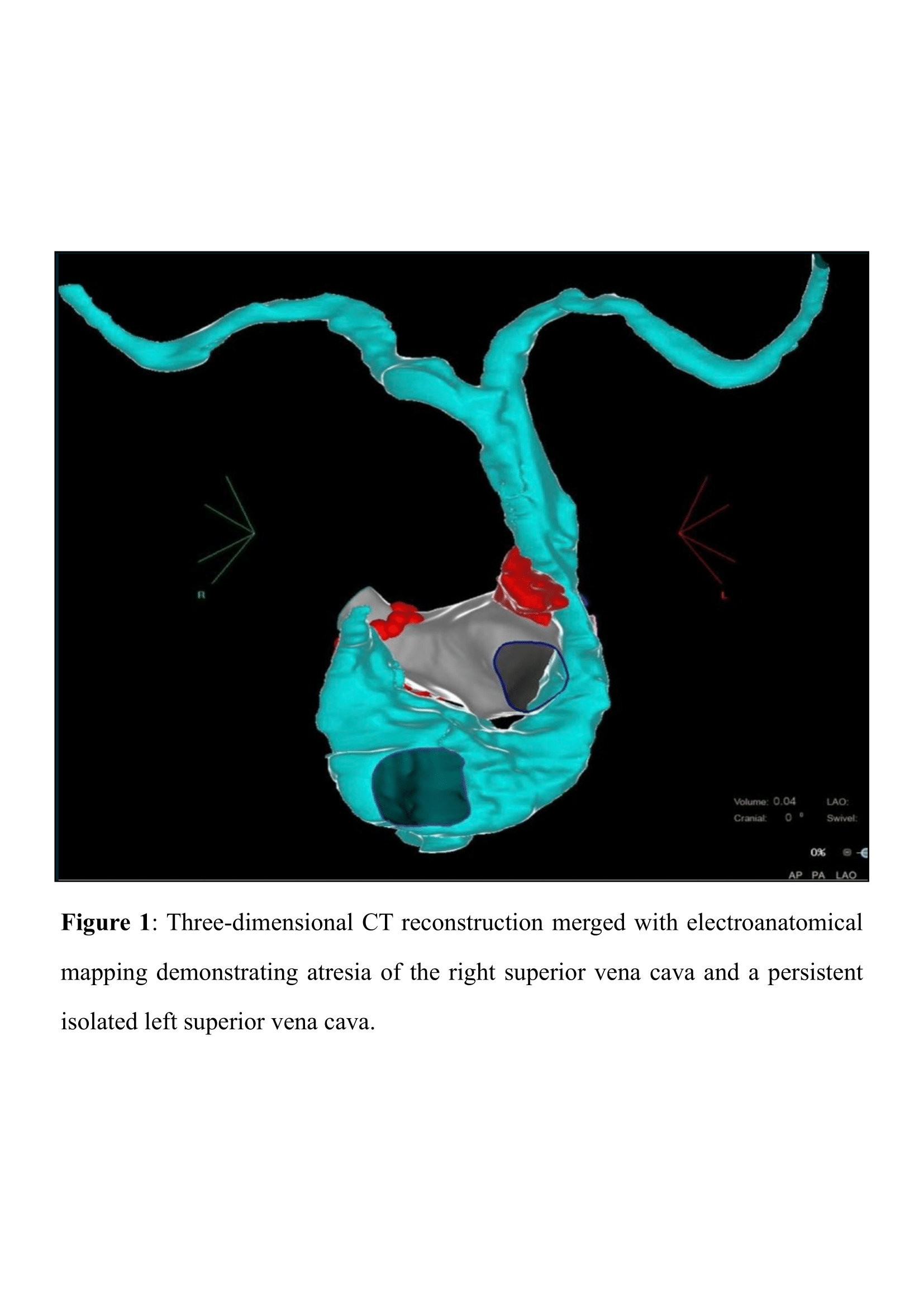
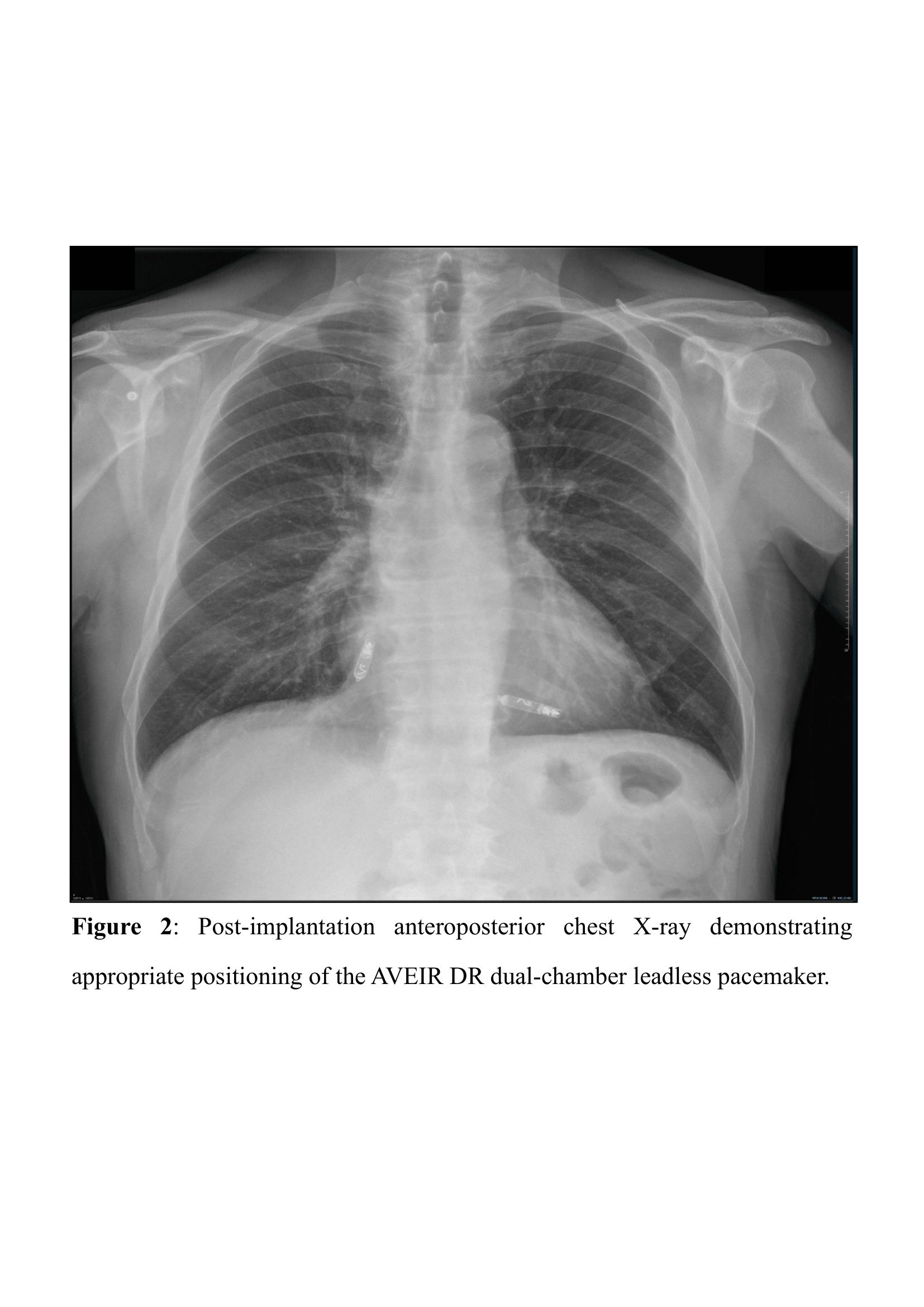
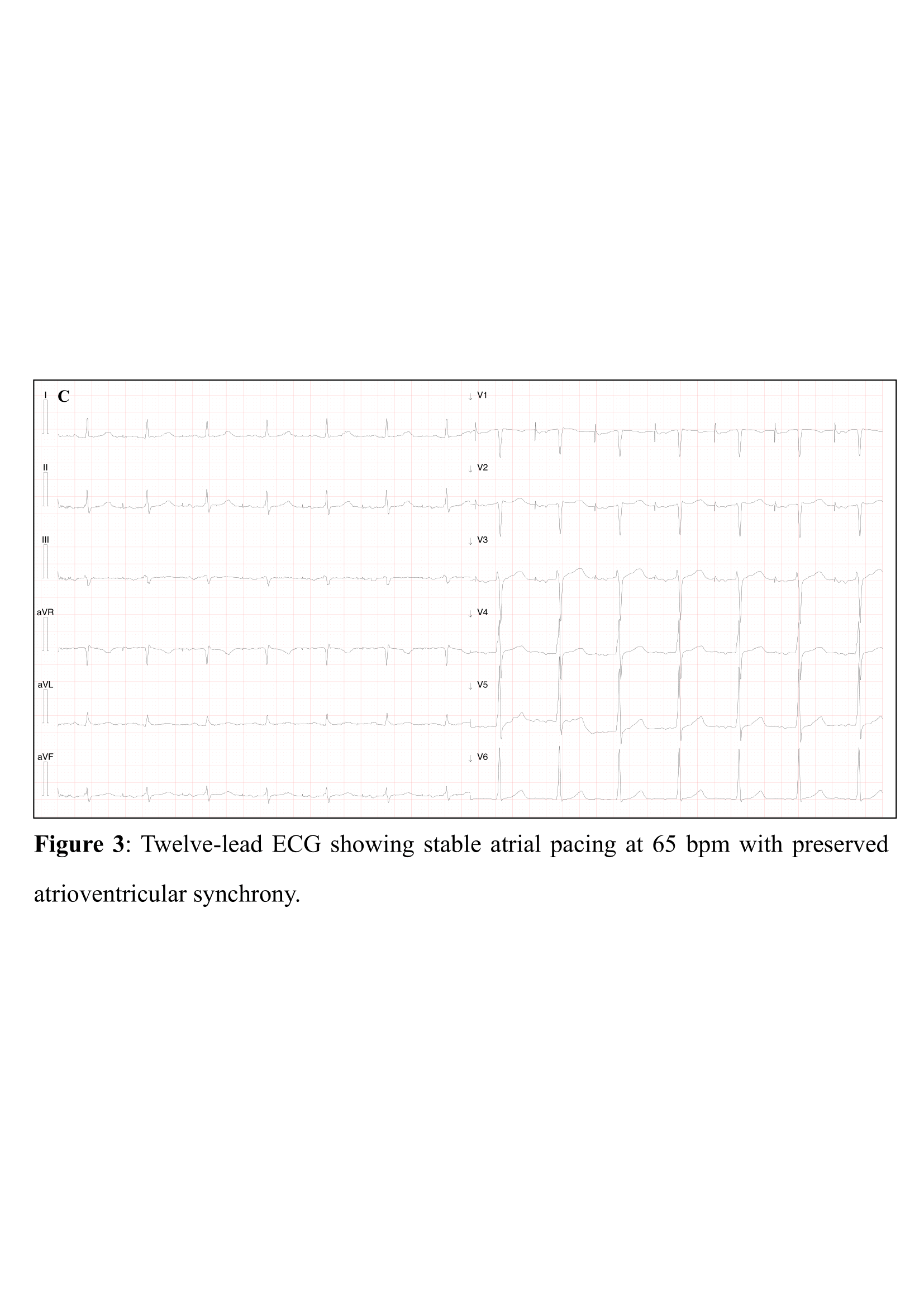
A 67-year-old man was referred for catheter ablation and permanent pacing due to symptomatic bradycardia–tachycardia form of sinus node dysfunction (SND), characterized by paroxysmal atrial fibrillation (AF), intolerance to antiarrhythmic therapy related to sinus bradycardia and chronotropic incompetence. Transthoracic echocardiography demonstrated preserved left ventricular systolic function and a markedly dilated coronary sinus (CS). Contrast-enhanced computed tomography revealed a persistent left superior vena cava (LSVC) draining into the CS, with congenital absence of the right superior vena cava, consistent with isolated LSVC (ILSVC). After 3D reconstruction of the left atrium and LSVC, bilateral complete first-pass pulmonary vein isolation was achieved without complications. Because of persistent sinus bradycardia and unfavorable venous anatomy, dual-chamber leadless pacemaker implantation was planned a few months later. Under general anesthesia and transesophageal echocardiographic (TEE) guidance, the ventricular leadless device was implanted in the right ventricular (RV) apical septum via the right femoral vein. After right atrial (RA) angiography, the atrial leadless device was positioned in the RA appendage. Post-procedural TEE confirmed correct device positioning, with no pericardial effusion or tricuspid regurgitation. Device interrogation showed stable electrical parameters: RA sensing 4.8 mV, threshold 0.5 V at 0.4 ms, impedance 400 Ω; RV sensing 9 mV, threshold 0.5 V at 0.4 ms, impedance 860 Ω. The system was programmed to AAIR 60 bpm with VVI backup at 40 bpm. Post-procedural chest X-ray confirmed correct device positioning, and the ECG showed atrial pacing at 60 bpm. At one-month follow-up, the patient reported symptomatic improvement with stable atrial pacing and normal device function. ILSVC is a rare congenital anomaly associated with increased risk of AF and SND and poses significant challenges for conventional transvenous pacing due to complex venous anatomy. Leadless pacing systems overcome these limitations by avoiding transvenous leads. Moreover, the dual-chamber leadless system enables true physiological atrioventricular pacing through inter-device communication, addressing the limitations of earlier first-generation leadless systems. This case demonstrates the feasibility and safety of dual-chamber leadless pacemaker implantation in ILSVC, supporting its role in patients with complex venous anatomy requiring permanent pacing.