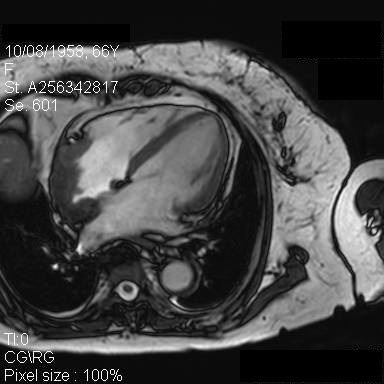
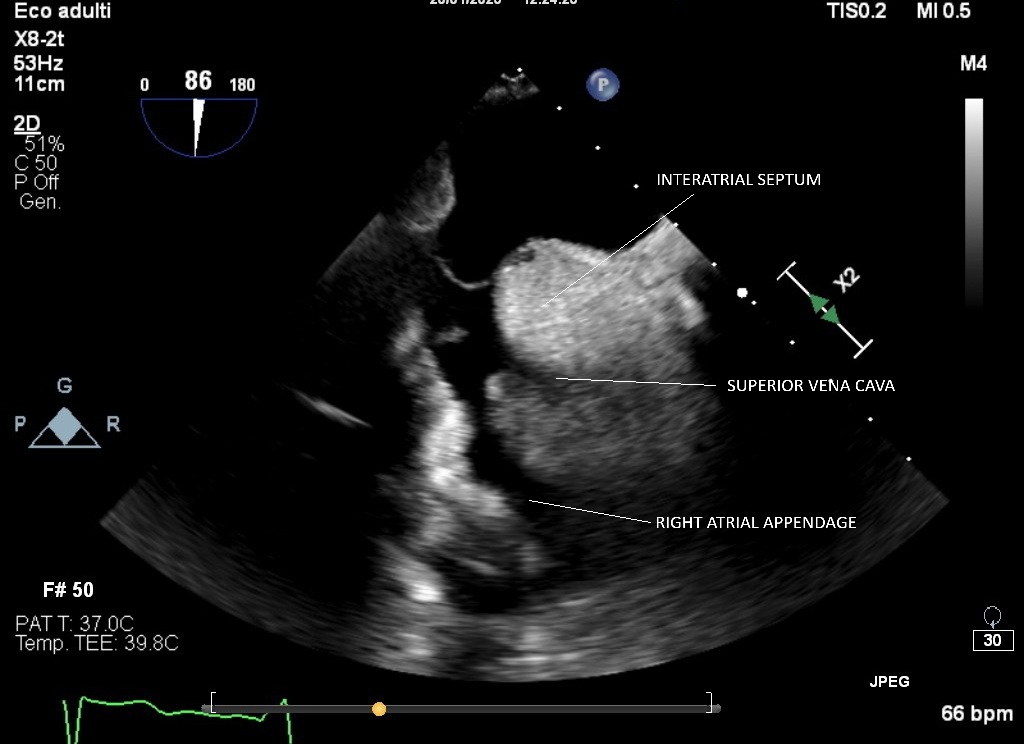
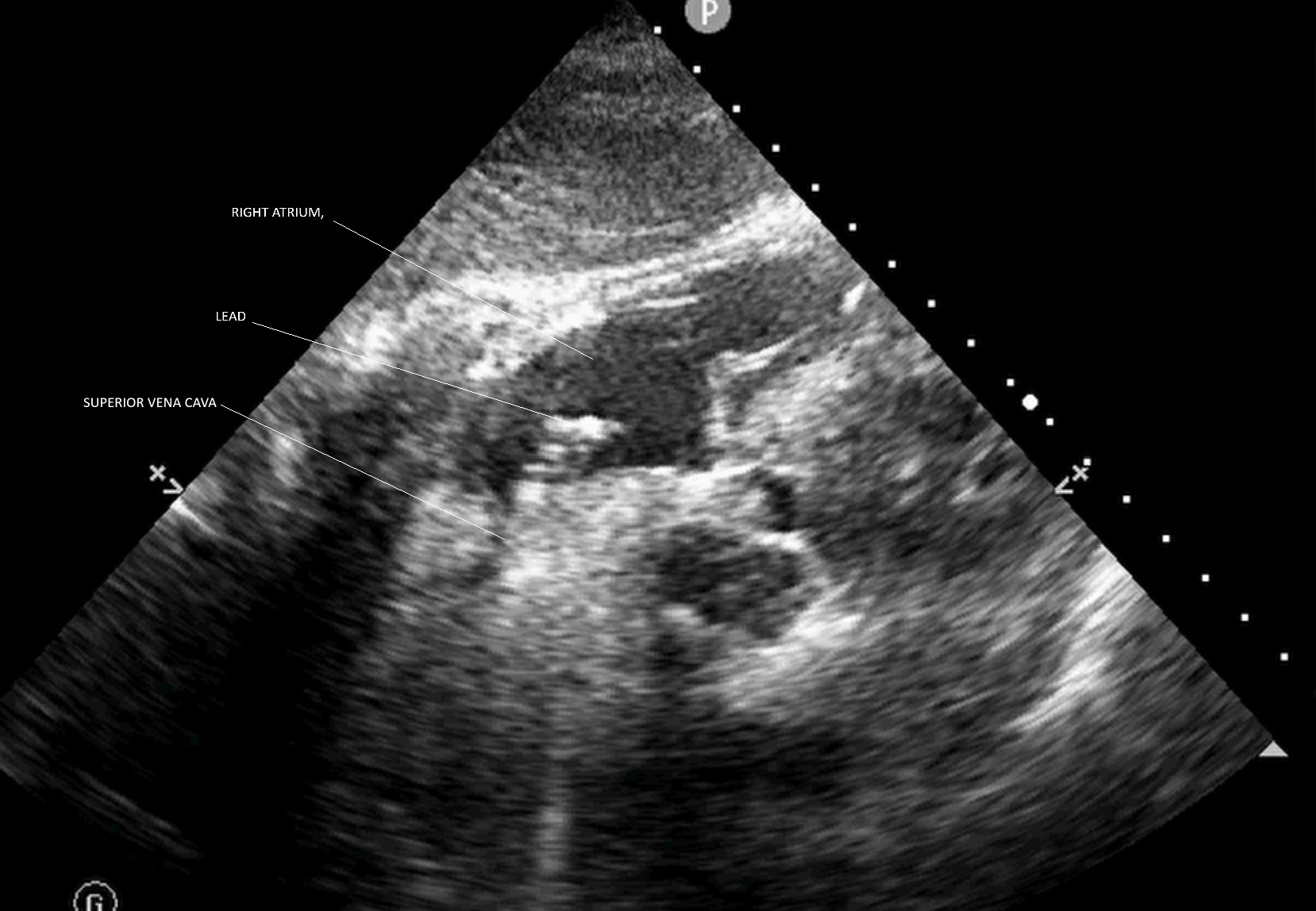
Erdheim–Chester disease (ECD) is a rare systemic non- Langerhans cells histiocytosis of unknown etiology characterized by multiorgan xanthomatous infiltration by foamy histiocytes. Cardiovascular involvement in ECD is frequent, at level of the right atrium and superior vena cava. We present the case of a 67-year-old woman with history of ECD and cardiac involvement, referred to our attention following syncopal episodes and paroxysmal atrial fibrillation alternating with phases of marked sinus bradycardia and asystolic pauses. Transesophageal echocardiogram and cardiac MRI (Fig 1) confirmed the increased wall thickness and the marked reduction of the internal diameter of the superior vena cava and of the right atrium. The clinical cardiological problem was the need to submit the patient to the implantation of a dual-chamber pacemaker for sick sinus syndrome. Despite the stenosis at the level of the superior vena cava and the involvement up to the brachiocephalic veins, we decided to try an implant with a traditional approach from the left axillary vein, aiming for a dual-chamber stimulation, following the procedure with fluoroscopic and ultrasound guidance. The ultrasound images also showed that the right atrial appendage appeared spared by the disease and with regular thicknesses (Fig 2), thus representing a good target where insert the atrial lead . During pacemaker implantation, we followed the passage of the two leads at the level of the stenosis with ultrasound and fluoroscopic imaging, limiting the risk of complications, given the resistance and the need to force the push using more rigid stylets (Fig 3). P articularly delicate t he positioning of the active fixation electrode in the atrium (the area most affected by histiocytosis) , where ultrasound guidance was useful for the control of any bleeding or perforation of the electrode. The implantation was completed without complications and the electrical parameters of the pacemaker were optimal . This case confirms how a multimedial imaging approach is crucial to organize and best perform electrostimulation procedures in particular anatomical contexts such as in ECD with cardiac involvement, minimizing the risks.