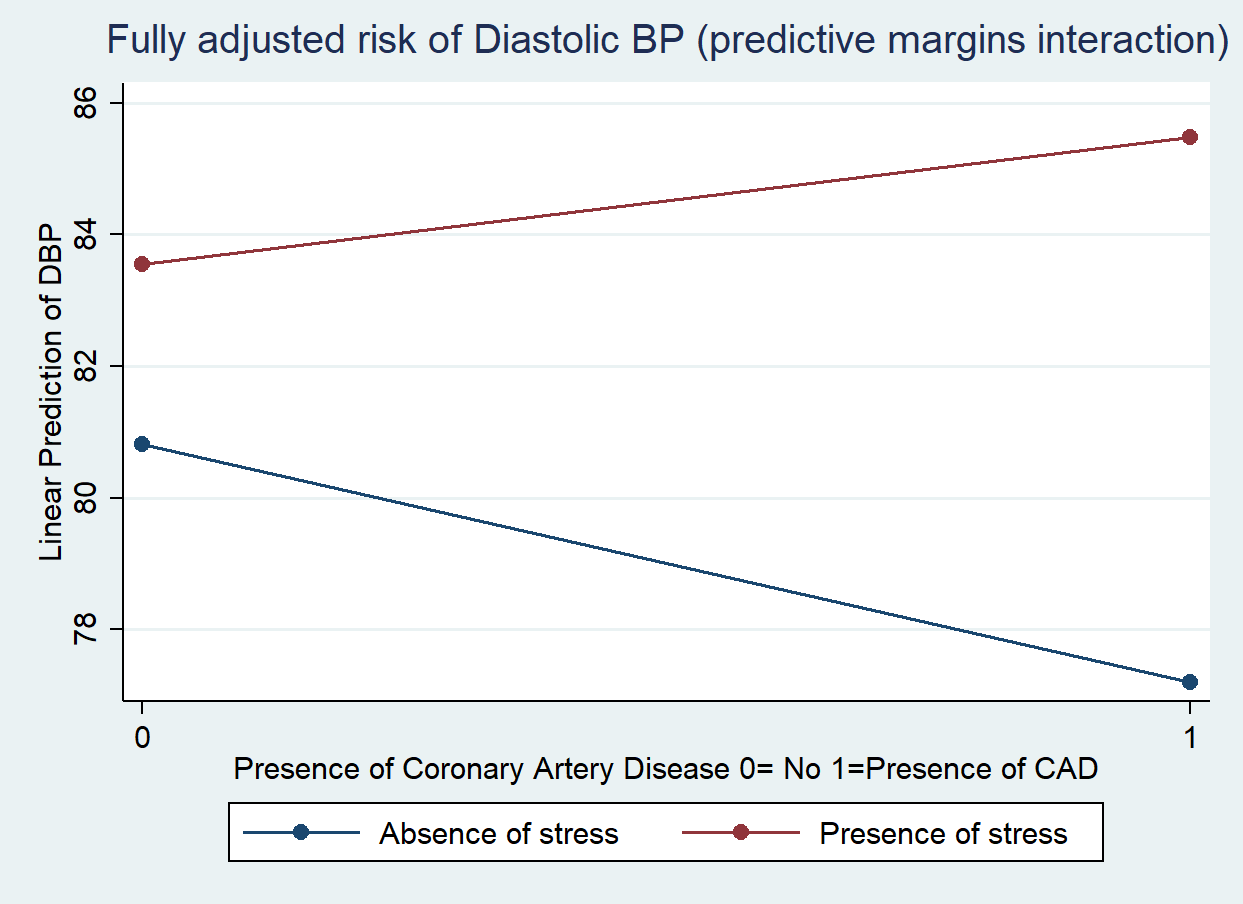
Background: Psychological stress has emerged as a significant non-traditional driver of cardiovascular disease (CVD). Despite its clinical relevance, the quantitative association between stress levels and objective hemodynamic markers in diverse patient populations remains to be fully elucidated. This study aimed to evaluate the relationship between perceived stress and blood pressure parameters within a large, multicenter cohort. Methods: We conducted a cross-sectional study across three clinical centers, enrolling 685 patients. Stress was defined based on standardized patient self-declaration. Blood pressure (BP) was assessed using the average of two consecutive measurements of systolic (SBP) and diastolic (DBP) blood pressure, taken five minutes apart. Statistical analysis utilized multiple linear regression models. Starting from a full model adjusting for key confounders (age, sex, physical activity, and CV risk factors including smoking, diabetes, and antihypertensive threatment), a parsimonious model was derived to identify the most significant independent predictors of BP. Interaction terms were tested to evaluate the moderating effects of clinical variables. All analyses were carried out using STAT 18.0 StataCorp LLC, (TX) USA. Results: In the multivariate analysis, perceived stress emerged as a significant independent predictor of increased DBP (β=3.5 ± 0.8 ; t=4.2; p<0.0001), whereas no significant association was observed with SBP. While Coronary artery disease (CAD) was not an independent predictor of BP in the initial models, the introduction of an interaction term revealed a significant positive interaction between stress and CAD (β=6.5 ± 02.3 ; t=2.4; p=0.01). Specifically, the impact of psychological stress on DBP levels was significantly more pronounced in patients with a history of CAD compared to those without. Conclusions: The specific association between stress and DBP suggests that psychological stress may primarily influence cardiovascular hemodynamics by increasing basal sympathetic activity and peripheral vascular resistance. In clinical practice, screening for stress is essential, particularly in patients with CAD, as they exhibit heightened hemodynamic sensitivity to psychological factors. Stress management should be considered a key component of cardiovascular risk stratification and secondary prevention.