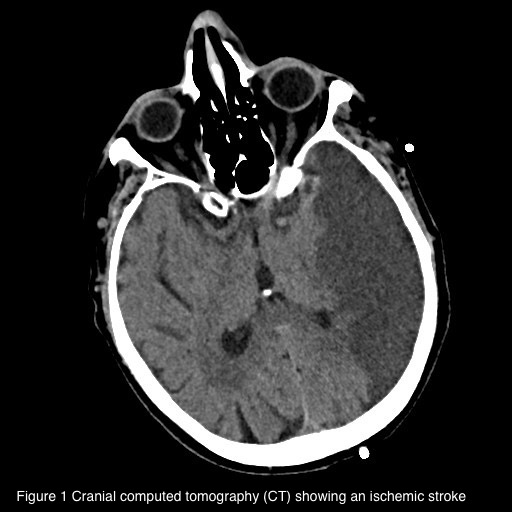
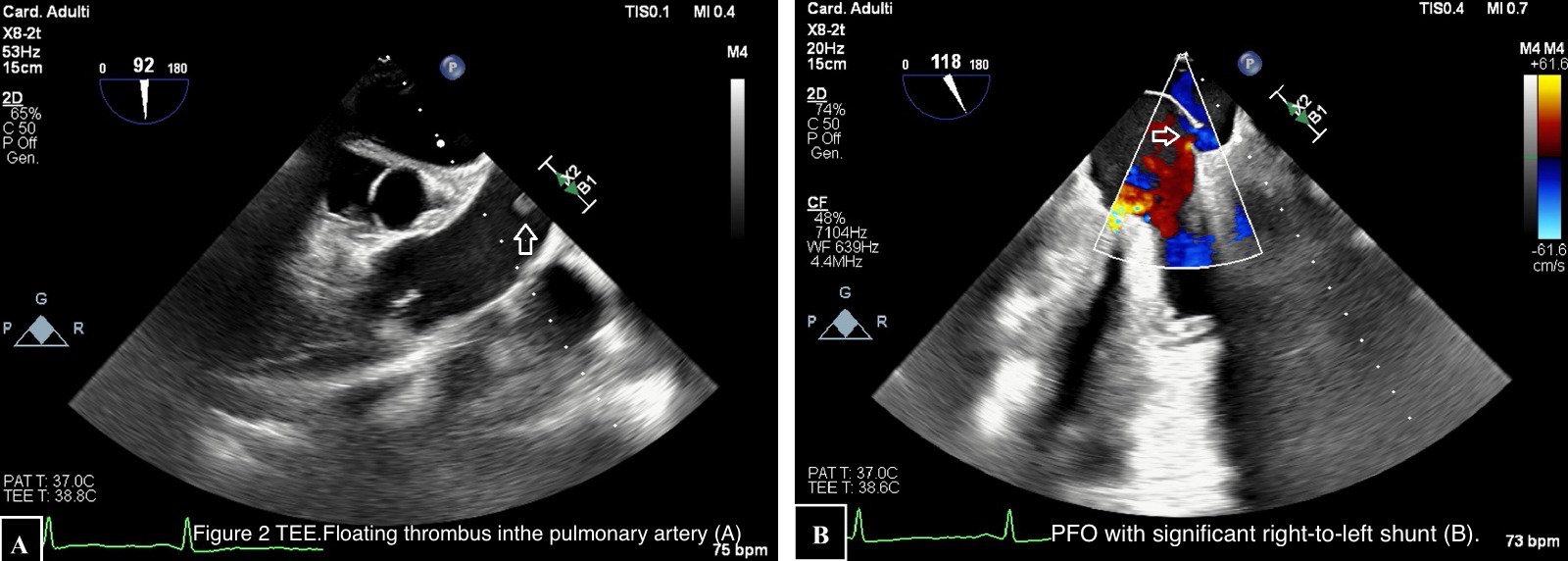
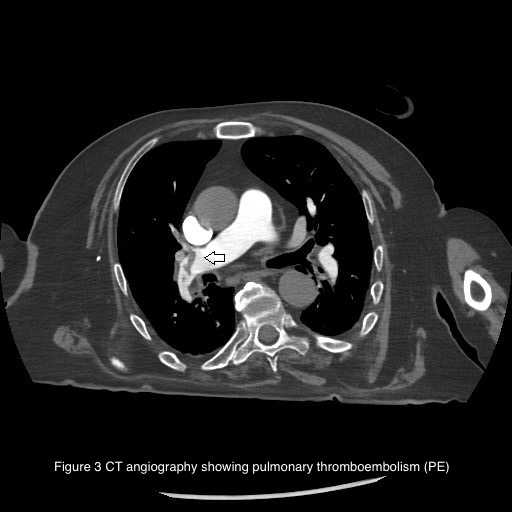
Introduction Ischemic stroke (IS) is caused by the obstruction of cerebral blood vessels, resulting in reduced blood flow and impaired oxygen delivery. It can be caused by atherothrombotic occlusion of large arteries, cerebral embolism or non-thrombotic occlusion of small, deep cerebral arteries. Cardioembolic IS can occur in the presence of various cardiac conditions, such as cardiac masses, patent foramen ovale (PFO), endoluminal thrombosis and sometimes as complication of infective endocarditis (IE). We present the case of a patient admitted to Intensive Care Unit (ICU) after non-cardiac surgery (NCS) who developed IS with high suspicioun of cardioembolic origin. Case presentation A 67-year-old man admitted to ICU developed right-sided hemiparesis after laparoscopic enterolysis surgery. His past medical history included a previous intestinal resection for ischemia. Computed tomography (CT) confirmed IS (1) , suspicious for embolic origin. Atherosclerosis of large cerebral vessels was excluded. Due to post-operative fever, blood cultures were collected and an infection caused by S. Aureus and M. Morganii was detected. Transoesophageal echocardiogram (TEE) was performed to confirm the suspicion of IE with embolization. TEE showed PFO with a significant right–to-left shunt (2B) . Moreover, a floating thrombus was detected in the pulmonary artery (2A) . No IE was found. CT angiography confirmed pulmonary thromboembolism (PE) (3) . Unfortunately, the patient died because of post-operative complications. Discussion The peculiarity of this case is represented by the unexpected aetiology of IS considering the clinical confounding presentation. At first, the most probable expected cause was represented by IE but PE and paradoxical embolization due to large PFO turned out to be responsible of IS. Some studies demonstrate PFO association with increased risk of IS in patients undergoing NCS in different settings. The prevalense of PFO in the general population is estimated at approximately 20-25% but the lack of a systematic screening in patients without IS likely underestimates its prevalence. Currently, PFO closure in addition to anti-aggregation therapy is indicated in patients with IS when a strong causal relationship between PFO and stroke is demonstrated. Further prospective trials are needed to identify a specific population at risk of perioperative IS associated with PFO in order to define systematic screening, prevention plans and improve perioperative outcomes.