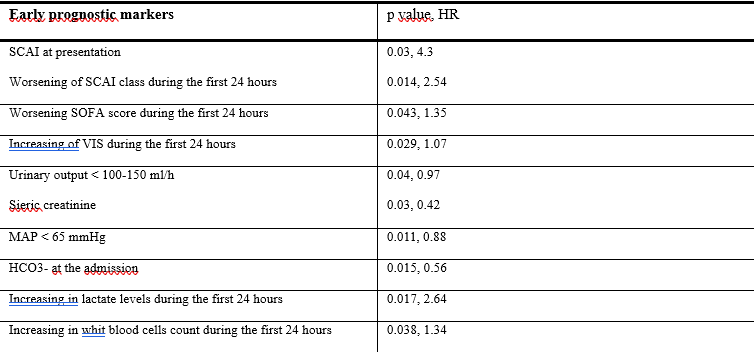
Background: cardiogenic shock (CS) remains associated with high in-hospital mortality despite therapeutic advances. Early identification of patients at risk of deterioration is essential for timely escalation of therapy. Aims: the aim of this prospective observational study was to identify early markers of clinical deterioration associated with high in-hospital mortality, enabling prompt escalation of pharmacologic and non-pharmacologic therapy. Methods: this study consecutively enrolled 20 patients admitted to the Intensive Cardiac Care Unit of a tertiary center for CS from February to August 2025. Daily multimodal monitoring was performed to identify early markers of poor prognosis by assessing clinical (systolic and mean arterial pressure, SOFA score), laboratory (white blood cell count, AST, ALT, serum creatinine), blood gas (SvO₂, arterial lactate, serum bicarbonate, arterial–venous pCO₂ gap), echocardiographic (ejection fraction, indexed stroke volume, cardiac index), and invasive hemodynamic (indexed stroke volume and cardiac index) parameters. These variables were compared according to outcome, with emphasis on in-hospital mortality, and their changes during the first 24 hours were also evaluated. The impact of these parameters on in-hospital mortality and time to recovery was assessed using Cox proportional hazards regression. Results: l ower mean invasive arterial pressure (MAP) at admission (p = 0.011, HR 0.88) and urine output < 150 mL/h (p = 0.04, HR 0.97) were associated with higher in-hospital mortality, as well as higher creatinine levels (p = 0.03, HR 0.42). Poorer outcomes were seen in patients with higher SCAI class (p = 0.03, HR 4.3), SOFA score (p = 0.043, HR 1.35), and Vasotropic–Inotropic Score (p = 0.029, HR 1.07), and in those whose SCAI class increased within the first 24 hours from diagnosis (p = 0.014, HR 2.54). Low serum bicarbonate levels at the onset of CS were associated with increased in-hospital mortality (p = 0.015, HR 0.56) as well as rising in serum lactate levels (p = 0.017, HR 2.64), and higher white blood cells count (p = 0.038, HR 1.34) within the first 24 hours. Conclusions: dynamic monitoring of early markers of hypoperfusion and systemic inflammation, rather than single absolute values, allows timely identification of patients at risk of CS deterioration and may serve as a clinical decision-support tool.