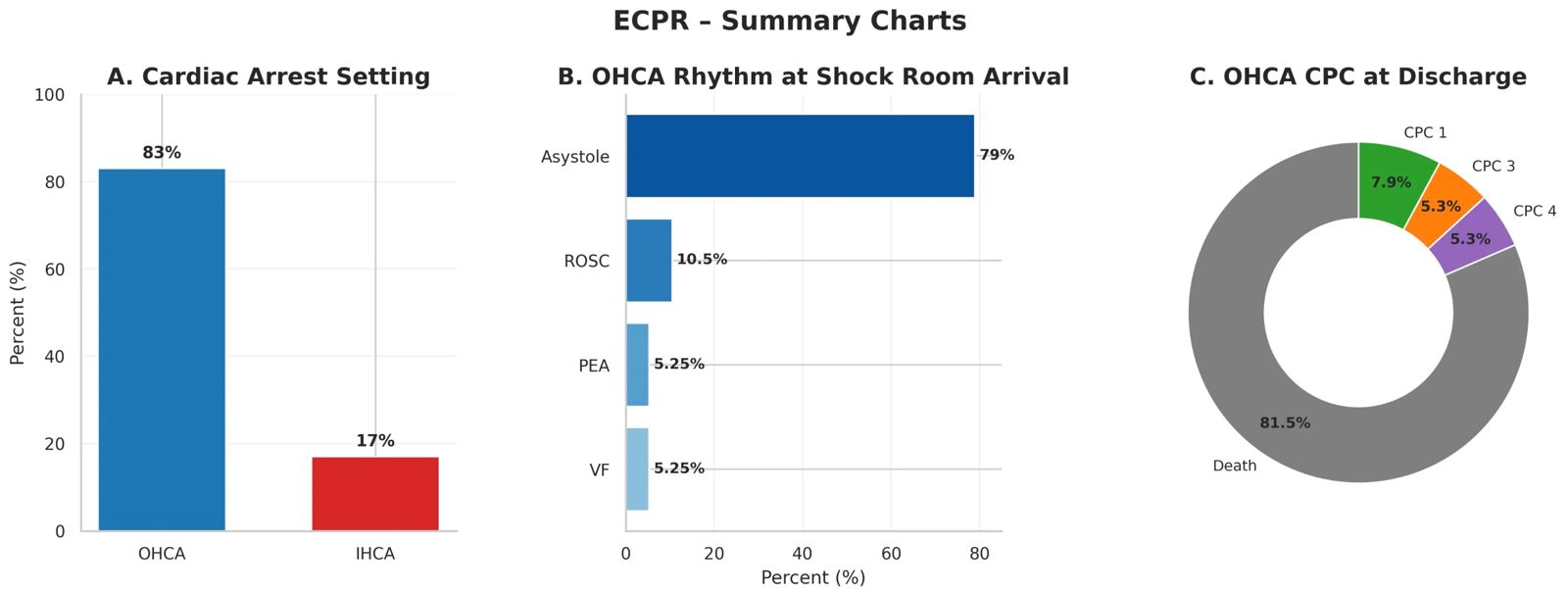
Background : Out-of-hospital cardiac arrest (OHCA) is associated with high mortality and poor neurological outcomes despite advances in emergency cardiovascular care. Extracorporeal cardiopulmonary resuscitation (E-CPR) has emerged as a rescue strategy for selected patients with refractory cardiac arrest. In 2019, an E-CPR program was integrated into a pre-existing acute myocardial infarction (AMI) network. Objectives : To describe indications and clinical outcomes of patients treated with E-CPR at a tertiary referral ECMO center. Methods : We performed a retrospective, single-center observational study including all consecutive patients (n=46) who underwent E-CPR for OHCA or for in-hospital cardiac arrest (IHCA) related to acute myocardial infarction. Institutional inclusion criteria were age <70 years, shockable presenting rhythm, low-flow time <10 minutes, time from advanced cardiac care activation to shock room arrival <45 minutes, and time from cardiac arrest to ECMO flow <60 minutes. Demographic data, E-CPR indications, and outcomes were collected. Survival and neurological outcome were assessed at index hospital discharge using the Cerebral Performance Category (CPC) scale. Results : Forty-six patients (median age 61 years) received E-CPR: 38 (83%) for OHCA and 8 (17%) for IHCA. Median ECMO duration was 2 days. Among OHCA patients, cardiac rhythm at shock room arrival was return of spontaneous circulation (ROSC) in 4/38 (10.5%), pulseless electrical activity in 2/38 (5.3%), ventricular fibrillation in 2/38 (5.3%), and asystole in 30/38 (79%). At hospital discharge, CPC among OHCA patients was CPC 1 in 3/38, CPC 3 in 2/38, and CPC 4 in 2/38. Overall survival was 13/46. Among survivors, CPC was 1 in 7 patients, 3 in 2 patients, and 4 in 2 patients. Favorable neurological outcome (CPC 1–2) was observed in 6/13 survivors (46%). Conclusions : In this single-center experience, E-CPR was associated with survival and favorable neurological outcomes in a selected subgroup of patients despite high overall mortality. These findings support the role of E-CPR within organized regional systems of care.