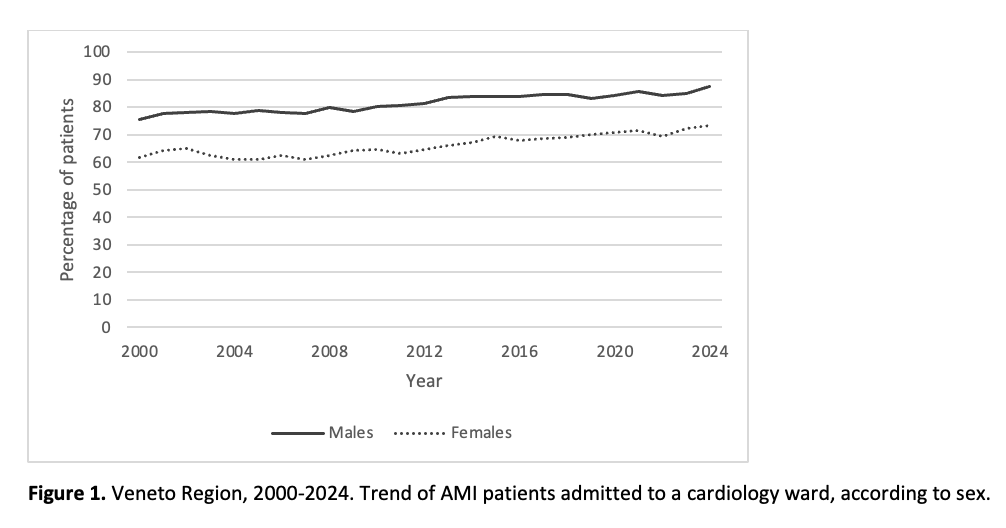
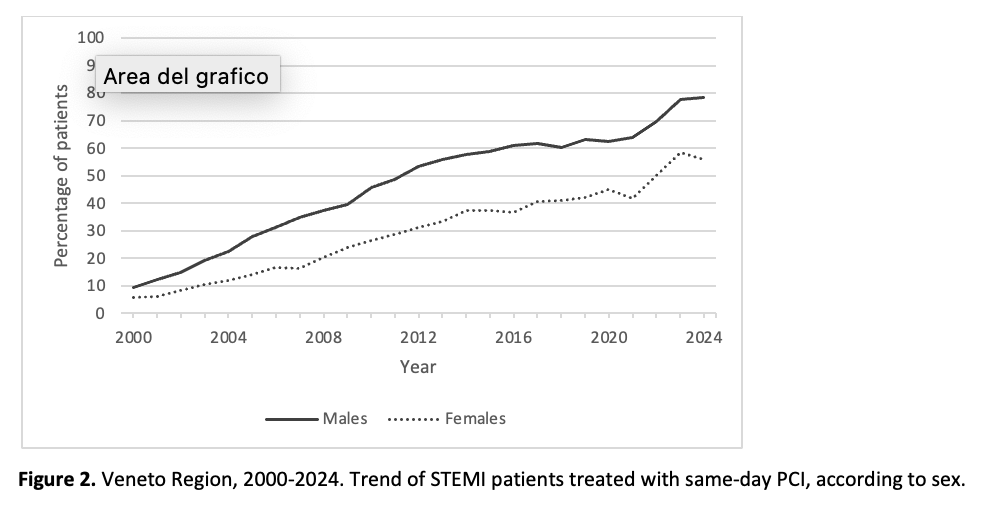
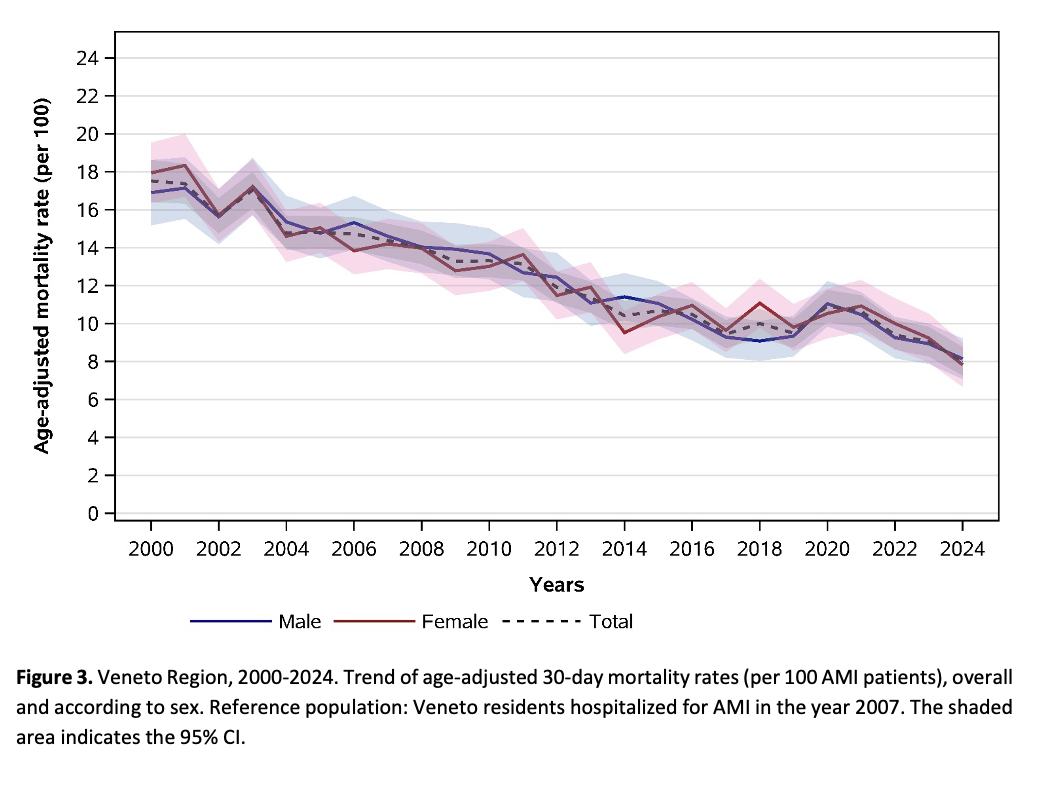
Aim Sex differences in the management and outcomes of patients hospitalized with acute myocardial infarction (AMI) had been reported worldwide. In this analysis, we aimed to examine this topic in the Veneto Region (Italy) through a 25-year population-based study. Methods We conducted a retrospective analysis of all hospital discharge records from 2000 to 2024 in the Veneto Region, identifying AMI cases through ICD9-CM codes. The proportion of AMI patients hospitalized in a cardiology ward (ordinary or intensive care) and the proportion of same-day percutaneous coronary intervention (PCI) among ST-Elevation myocardial infarction (STEMI) cases, as well as 30-day mortality, were estimated according to sex. Results Over the study period, 107,620 males (mean age: 68.0±13.1 years) and 59,657 females (mean age: 77.3±12.1 years) were hospitalized for AMI in the Veneto Region. Of these patients, 81.4% of males were admitted to a specialized cardiology ward compared to 65.7% of females (p<0.001), with a 13-18% sex-gap observed steadily over the entire time series ( Figure 1 ). The proportion of STEMI patients who underwent a same-day PCI was also higher in males compared to females (43.2% and 24.7% respectively), with a gap in favour of males that enlarged progressively during the first decade of the study and remained within the range 17-24% from 2010 onwards ( Figure 2 ). Both care process indicators showed an increase over time in both sexes, with a slight steeper increase among females. Crude 30-day mortality rate was 9.7% (95% CI: 9.5 to 9.9) for males and 17.1% (95% CI: 16.7 to 17.4) for females. Age-adjusted mortality rate was 12.5% (95% CI: 12.3 to 12.8) for males and 12.9% (95% CI: 12.6 to 13.2) for females. A continuous decline might be observed in both sexes. ( Figure 3 ). Conclusions Sex differences in AMI management was observed in the Veneto Region from 2000 to 2024. However, the 30-day mortality rates overlapped throughout the entire time series after adjusting for age, suggesting that also the differences in management might be largely due to sex-difference in age at diagnosis. Care process indicators increased in both sexes reflecting the progressive implementation of standardized care pathways.