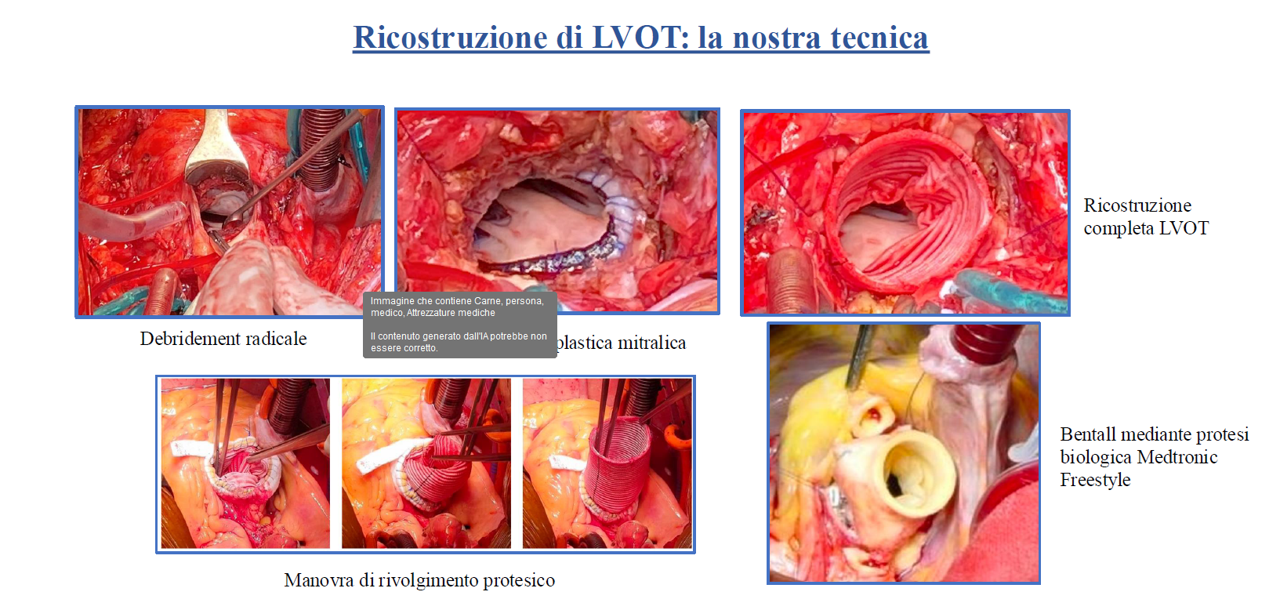
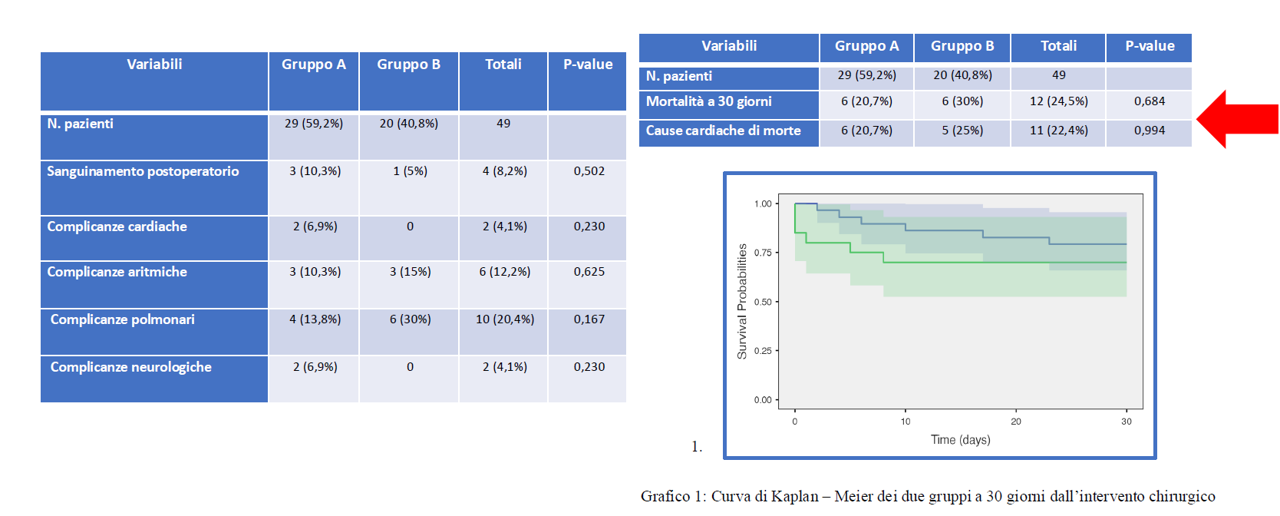
Background. Complex aortic valve endocarditis is one of the most feared complications of infectious endocarditis and, despite early diagnosis and treatment, it is still associated with a high rates of mortality and morbidity. Multicenter studies report 15-20% of in-hospital mortality and 40% of one-year mortality rate after surgery. It is characterized by the uncontrolled extension of the infectious process to the aortic root, perivalvular and sub-valvular structures, such as the left ventricular outflow tract, the mitro-aortic continuity zone and the fibrous skeleton of the heart. If the anatomical picture has not been excessively altered by the inflammatory-infectious process, aortic valve replacement represents the first-choice intervention and the one most performed throughout the world. In cases of locally invasive and destructive endocarditis, such as in the presence of extensive abscesses, it is necessary to replace the aortic root and, sometimes, associate a reconstruction of the partial or complete left ventricular outflow tract (LVOT). Despite the complexity of the operation, there are no detailed guidelines. The aim of our study was to evaluate the medium-term clinical results obtained in the group of patients undergoing complex surgical treatment using our specific technique and compare them with those obtained in the group of patients undergoing simpler surgical treatments, carrying out an evaluation according to international literature data. Methods . 49 patients underwent cardiac surgery for infective endocarditis (IE) divided into two groups: group A – Simple IE (29 patients) in which we performed valve replacement, valve repair and aortic root surgery; group B – Complex IE (20 patients), instead, in which we performed extensive surgical treatment with aortic root replacement, associated in 12 cases to the LVOT reconstruction (figure 1) , using a complete mitral prosthesis ring and a Dacron vascular prosthesis. Results. No statistically significant differences were found in terms of postoperative comorbidity, 30-day mortality, or follow-up mortality between patients with simple and complex endocarditis (figure 2) . Conclusion. Surgical treatment of complex endocarditis represents a difficult challenge for the cardiac surgeon, in relation to the extent of the infectious process and the consequent difficulty in standardizing a surgical technique, these data demonstrate that the surgical technique that we used is safe and reproducible.