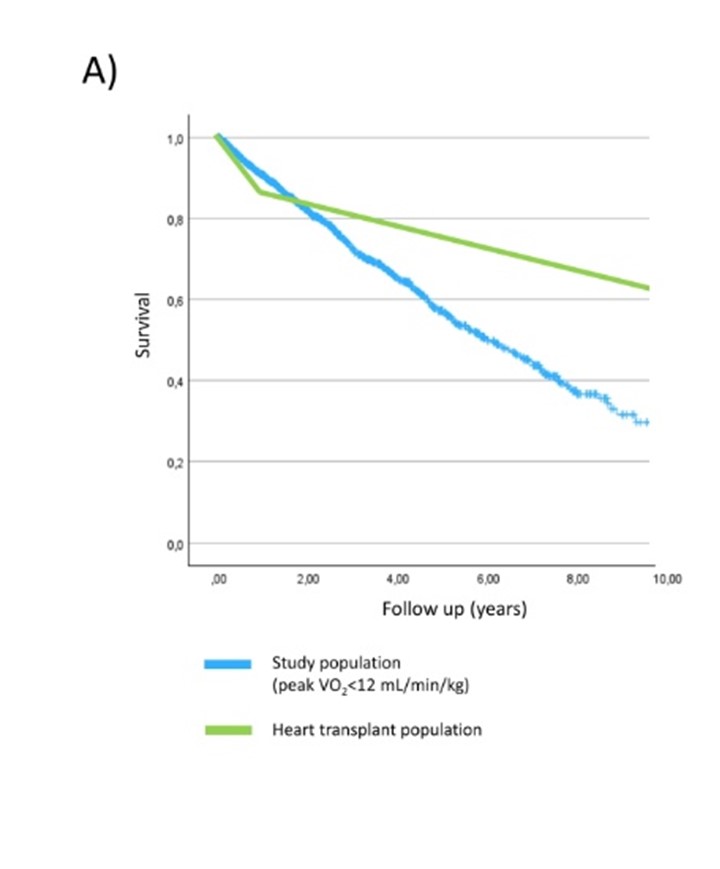
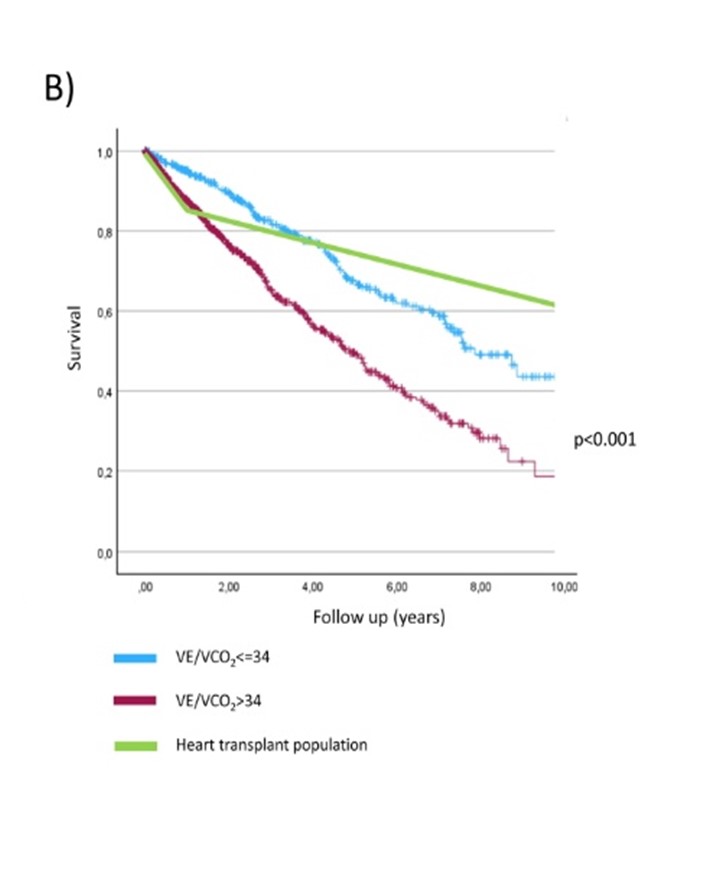
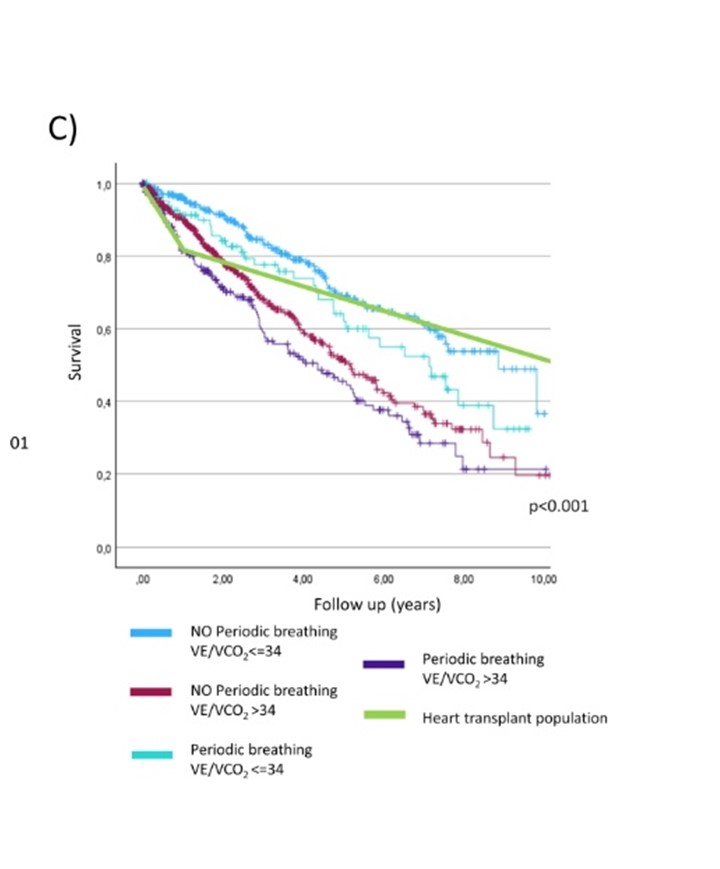
Background: Current guidelines recommend referring ambulatory heart failure (HF) patients for heart transplantation (HTX) when peak oxygen uptake (peak VO₂) is <12 mL/kg/min. This threshold, however, is based on decades-old data. As HF management has significantly improved, the relevance of this criterion in today’s clinical practice is uncertain. Methods: We retrospectively selected 1,218 ambulatory patients with HF and reduced or improved ejection fraction (HFrEF or HFimpEF) from the MECKI score registry, with peak VO₂ <12 mL/kg/min. Patients were enrolled between 2010 and 2022. Clinical and cardiopulmonary exercise testing (CPET) variables were recorded, with a primary composite outcome of death, LVAD implantation, or HTX. Kaplan-Meier survival curves were compared to contemporary data from heart transplant recipients in the ISHLT registry. We stratified patients by VE/VCO₂ slope (>34 vs. ≤34) and presence/absence of periodic breathing (PB). Sensitivity analyses included adjustment for % predicted peak VO₂ and subgroup evaluation in non-maximal CPET (RER <1.05). Results: Over a median follow-up of 2.3 years, 400 events occurred. Fig. 1A compares the survival of the study population with the survival of HTX recipients. Patients with VE/VCO₂ ≤34 (n=446) had significantly lower 10-year event rates than those with VE/VCO₂ >34 (26.2% vs. 37.2%, p<0.001). Survival in the VE/VCO₂ ≤34 group exceeded that of HTX recipients until year 4 (Fig. 1B). Similarly, absence of PB (n=884) was associated with improved outcomes (29.4% vs. 42.7%, p<0.001), with survival crossing HTX at year 3. Combining VE/VCO₂ and PB defined four distinct prognostic groups. Patients with both VE/VCO₂ ≤34 and no PB had the most favorable outcomes (10-year event rate 23.3%), surpassing HTX recipients at year 5 (Fig. 1C). Prognostic differences persisted after adjustment for % predicted peak VO₂ and were evident even in patients with RER <1.05. Conclusions: In a contemporary cohort, a peak VO₂ <12 mL/kg/min alone no longer identifies ambulatory HF patients with a high enough short-term mortality to justify transplant listing. Incorporating VE/VCO₂ slope and PB into CPET interpretation provides significantly improved risk stratification. These findings suggest that current HTX referral criteria might need revision to avoid premature listing of low-risk patients and target optimize organ allocation to patients with very poor prognosis.