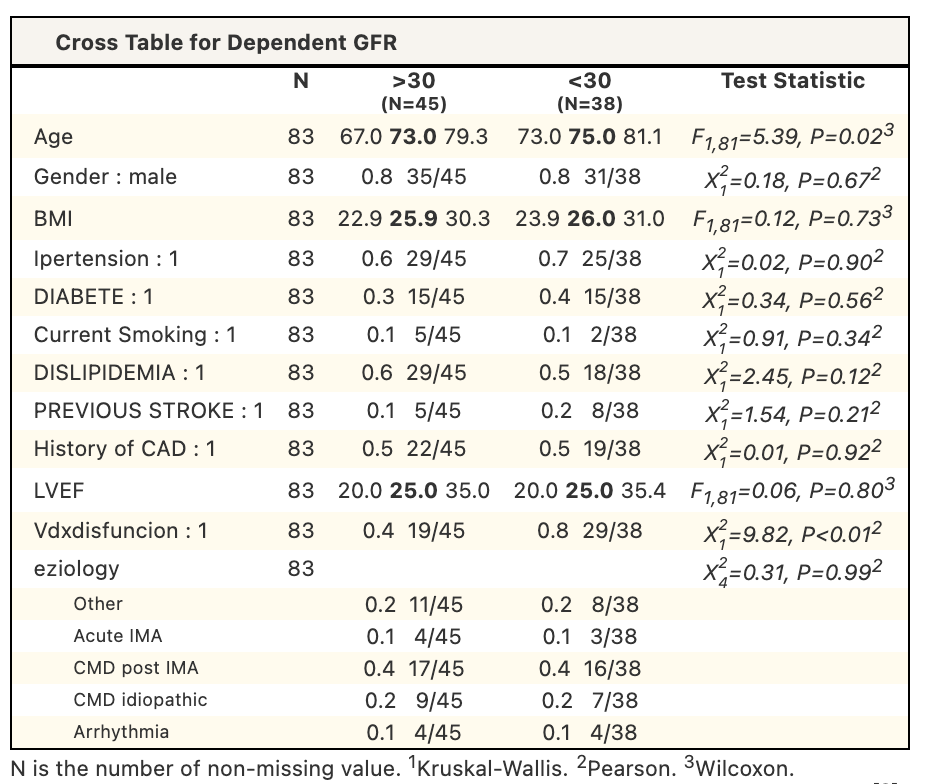
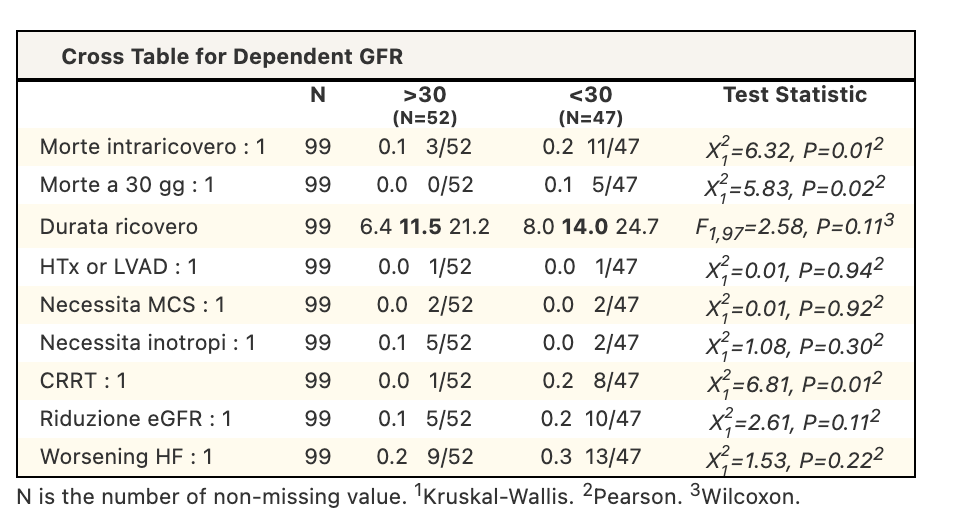
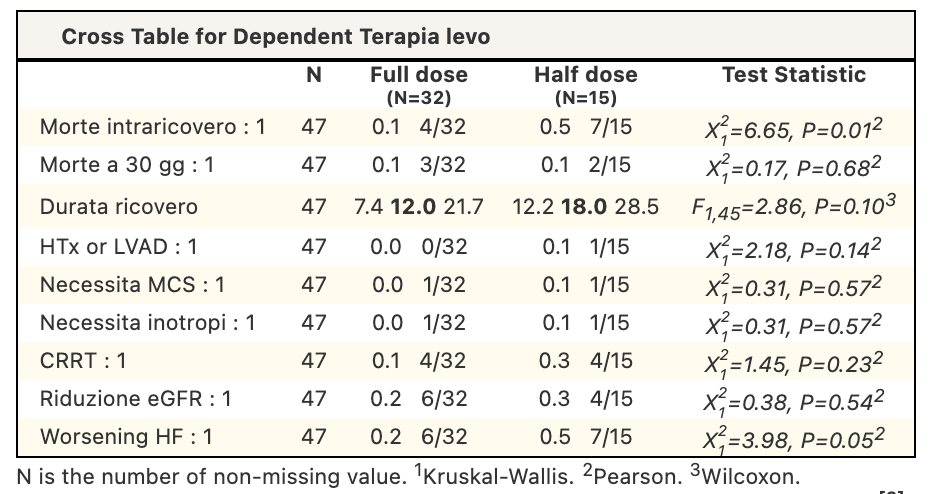
Acute heart failure and cardiogenic shock are often associated with renal dysfunction. While Levosimendan can have beneficial hemodynamic effects, its off-label use in patients with eGFR<30 mL/min requires caution due to limited evidence. This study aimed to evaluate clinical outcomes and treatment tolerability of levosimendan according to renal function. Methods : We conducted a retrospective observational study on patients treated with Levosimendan for acute heart failure or cardiogenic shock at Manzoni Hospital from July 2014 to July 2025. We divided patients into two groups based on renal function: eGFR <30 and ≥30 mL/min. Levosimendan was administered as a continuous infusion at 0.05–0.1 μg/kg/min over 24 hours, with the dose (12.5 mg or 6.25 mg) determined by the physician's judgment. Endpoints included in-hospital and 30-day mortality, hospital length of stay, renal function changes, need for renal replacement therapy, treatment tolerability, heart failure exacerbation, and inotropic support. A subanalysis compared outcomes in patients with eGFR <30 mL/min between the two dosages. Non-parametric and chi-square/Fisher’s exact tests were used (p <0.05). Results : Baseline characteristics based on renal function are shown in Table 1. Clinical outcomes by renal function are summarised in Table 2. Patients with eGFR <30 mL/min had higher in-hospital mortality, 30-day mortality and highterneed for continuous renal replacement therapy. In the sub-analysis of patients with eGFR <30 mL/min (Table 3), Overall outcomes were largely comparable between dosing strategies; however, higher in-hospital mortality and worsening heart failure were observed in the reduced-dose group. Conclusion: In our cohort, patients with severely reduced renal function who have been treated with Levosimendan showed a higher mortality and a greater need for renal replacement therapy, suggesting a more advanced clinical profile rather than reduced treatment tolerability. Within the subgroup of patients with eGFR <30 mL/min, differences in clinical outcomes were observed between full- and reduced-dose regimens; however, these findings should be interpreted with caution due to the non-randomised design and the likely influence of baseline disease severity on dose selection. Overall, levosimendan appeared feasible in patients with advanced renal dysfunction, and prospective studies are needed to clarify the impact of dosing strategies in this high-risk population.