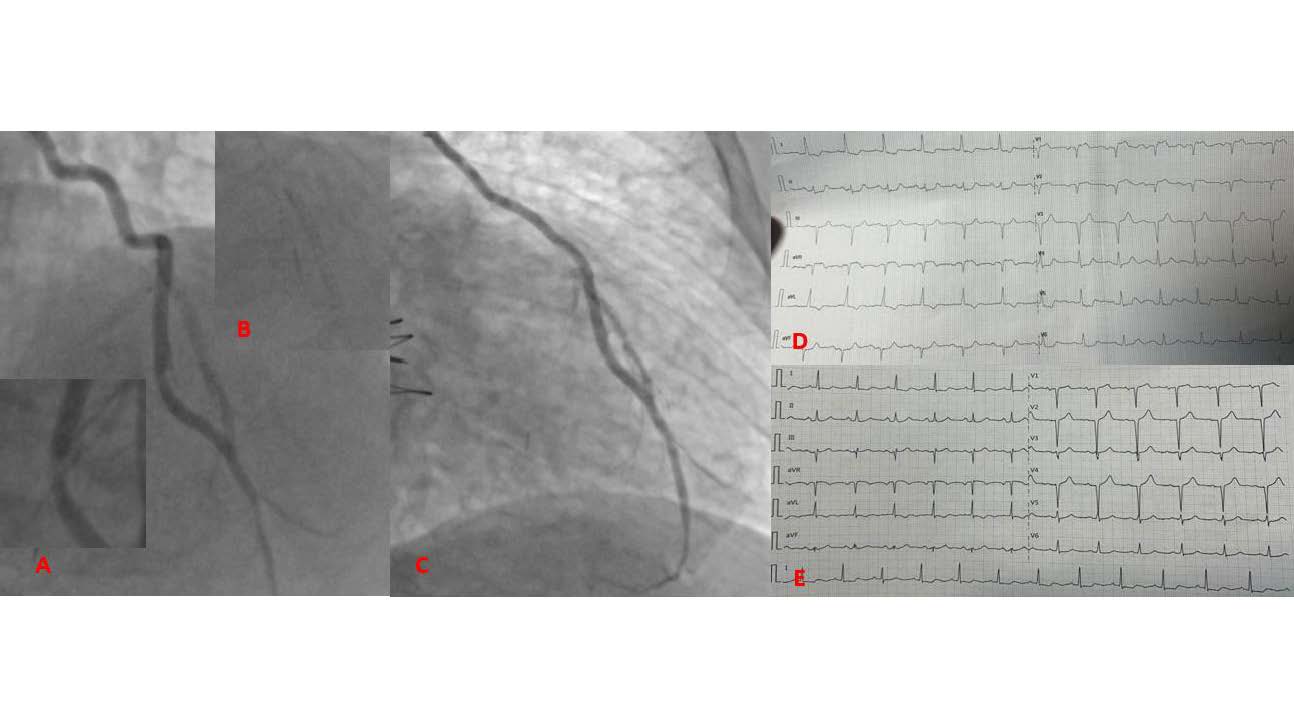
A 71 years old patients with an history of CABG with LIMA (left internal mammary artery) to LAD (left anterior descending artery) 20 years ago and multiple PCI was admitted to our department for prolonged rest angina (more than one hour) and vomit. The previous week he suffered from pneumonia. The ECG showed ST segment elevation of V1-V2 and aVR with specular ST segment depression of V4-V6 and DI-DII. He underwent urgent coronary angiography through left femoral artery which showed: “Three vessel coronary artery disease with CTO (chronic total occlusion) of proximal LAD and CTO of proximal RCA (Right coronary artery). Stent previously implanted on mid circumflex open without stenosis. VGS to CDX open without significant stenosis and a Left Internal Mammary Artery Graft to LAD with a severe dynamic stenosis on the mid-distal tract with contrast staining. LAD distal to LIMA had a significant stenosis”. The angiographic images of LIMA were pathognomic of spontaneous dissection. Considered the ongoing rest angina, the unstable emodinamics (blood pressure 90/60 mmHg) we performed emergent PCI through IM-catheter. The lesion was crossed with SION Blue coronary guidewire (0.014”). Wwe implanted three stent from mid-LAD to mid LIMA, overlapped (Biofreedom 2.75×29 mm, Biofreedom 3.0×33 mm and Coroflex Isar Neo 3.0×32 mm). Cardiovascular Snapshot. The editors will consider original, high-quality clinical images showing novel or “classic” findings for publication, subject to editing and revision. The image should not contain any material published elsewhere. All submissions should be accompanied by a cover letter. There should be no more than 6 authors. Maximum length: 150-word concise description, excluding the title, author list, figure legend, and references. There should be no more than 7 references. The figure should be consolidated into one multi-panel version. A graphical abstract (infographic) is mandatory. The graphical abstract must be submitted in PowerPoint format (see section 12 below for template).