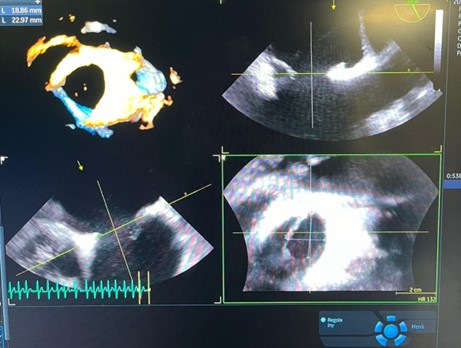
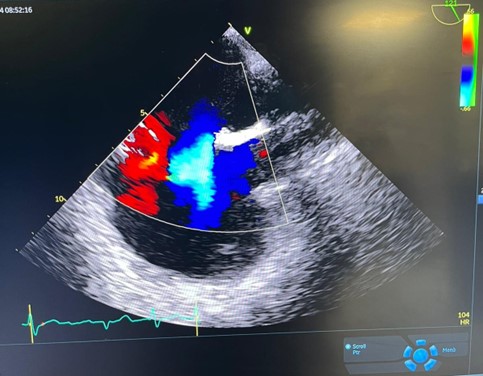
We described a case of a 75-year-old man, presented to the Emergency Department with intermittent chest pain. The electrocardiogram showed ST segment elevation in the inferior, posterior and right precordial leads. In consideration of the diagnosis of inferior-posterior STEMI, the patient was urgently transferred to the CathLab where coronary angiography revealed thrombotic occlusion of the mid-right coronary artery, treated with two drug-eluting stents. During the hospitalization, the patient underwent transthoracic echocardiogram which showed direct and indirect signs of pulmonary hypertension: dilated, hypertrophic and hypokinetic right ventricle, left ventricle D-shape (eccentricity index 0.8), dilated right atrium and signs of systemic venous congestion (dilated hypo-collapsible inferior vena cava and pulsatile portal venous flow with a Vexus score of 2). The interatrial septum was aneurysmatic, hypermobile, with a large ostium secundum type defect resulting in a left-to-right shunt. The diagnosis was confirmed by transoesophageal echocardiography, which showed bidirectional shunt. Then, the patient underwent right heart catheterization, which showed elevated pulmonary vascular resistances, contraindicating the immediate closure of the atrial septal defect. Therefore, the patient was referred to a tertiary center, where he started pharmacological therapy for pulmonary hypertension. Compared to the left ventricle, the right ventricle has lower afterload and lower wall stress and is infarct-resistant because it consumes a lower oxygen supply and has a higher oxygen reserve. There are some conditions, in which the right ventricle becomes more susceptible to ischemia, such as in right ventricular volume and pressure overload in large atrial septal defect, as it happened to our patient.