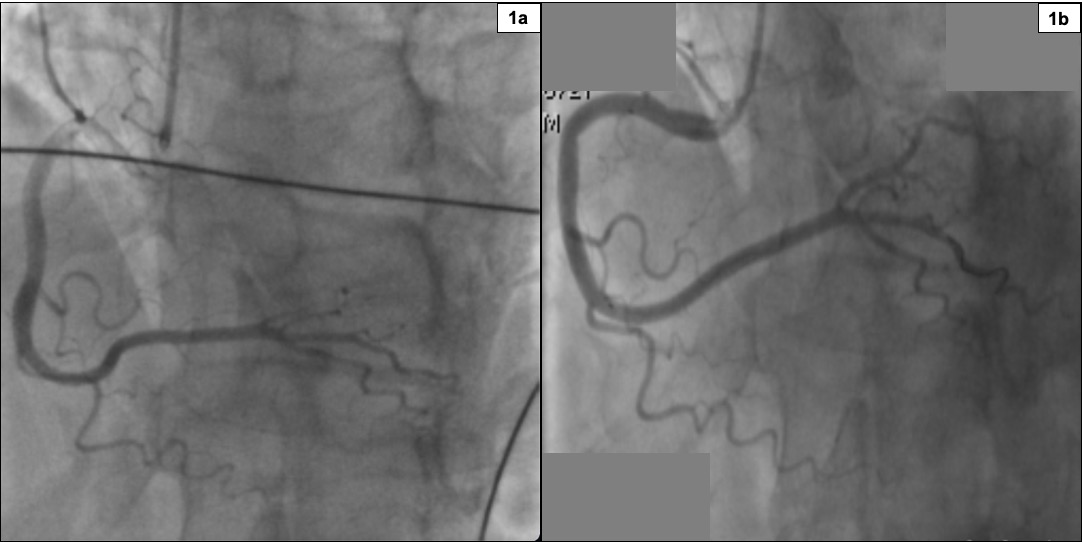
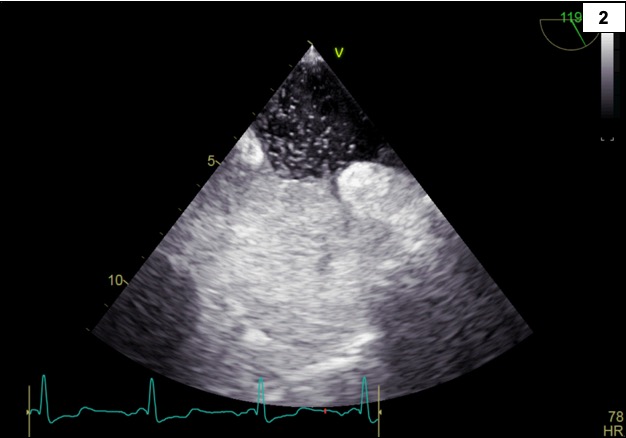
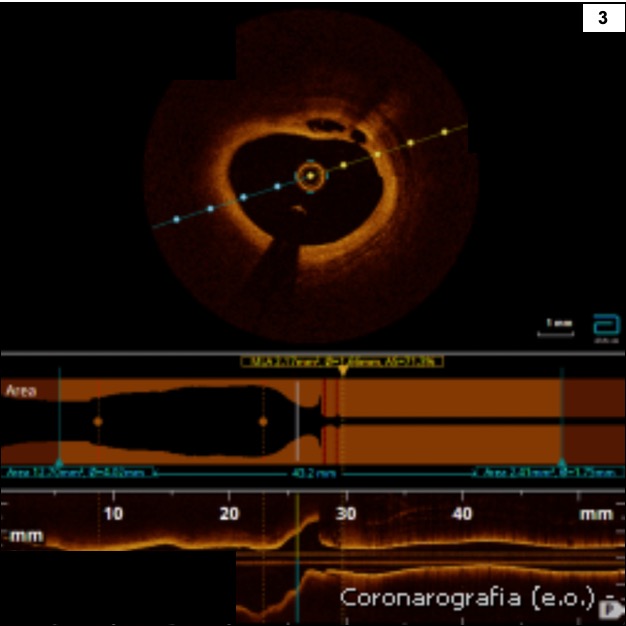
INTRODUCTION: Complications of non-stenotic unstable plaques, such as cracks, erosions, or ruptures, represent an insidious cause of ACS and are sometimes difficult to diagnose without the aid of intracoronary imaging. CLINICAL CASE: A 72-year-old male presented to the emergency department with persistent chest pain associated with cold sweating. His medical history included arterial hypertension, hyperuricemia, and CKD. The ECG was diagnostic for an infero-posterior STEMI, so the patient underwent primary PTCA. Coronary angiography revealed distal occlusions of the first and second posterolateral branches of the right coronary artery (RCA) (1a), likely of embolic nature, which were effectively revascularized with POBA PTCA (1b). Post-procedural echocardiography showed preserved LVEF with residual mild hypokinesia of the basal-inferior wall and preserved RV systolic function. Suspecting an embolic myocardial infarction (MI), ETE was performed, revealing a patent foramen ovale (PFO) with mild right-to-left shunt at baseline, and a large right-to-left shunt following a Valsalva maneuver (2). Anticoagulant therapy was started. However, lower limb venous Doppler ultrasound was negative for deep vein thrombosis. Despite the presence of PFO suggesting paradoxical coronary embolism likely cause of MI, the patient's advanced age, cardiovascular risk factors, and negative venous Doppler made a plaque-related complication more probable. Therefore, to identify possible unstable plaques that were activated but not causing significant stenosis, the patient underwent OCT imaging of the RCA. This revealed a plaque erosion near a moderate para-ostial stenosis (3). The coronary event was thus more likely attributed to distal embolization of a thrombus formed on the eroded plaque rather than a consequence of paradoxical embolism. Anticoagulant therapy was discontinued, and the patient was discharged with therapy including DAPT, statin, beta-blocker, and ACE-inhibitor. DISCUSSION: The presence of distal coronary thrombosis causing ACS, without significant proximal stenosis, can have multiple underlying causes. The detection of PFO with a large right-to-left shunt following a Valsalva maneuver could have been misleading, but appropriate clinical reasoning and the use of intracoronary imaging allowed for an accurate diagnosis. CONCLUSION: The use of intracoronary imaging was essential for accurately diagnosing plaque activation of a mild stenosis as a cause of ACS.