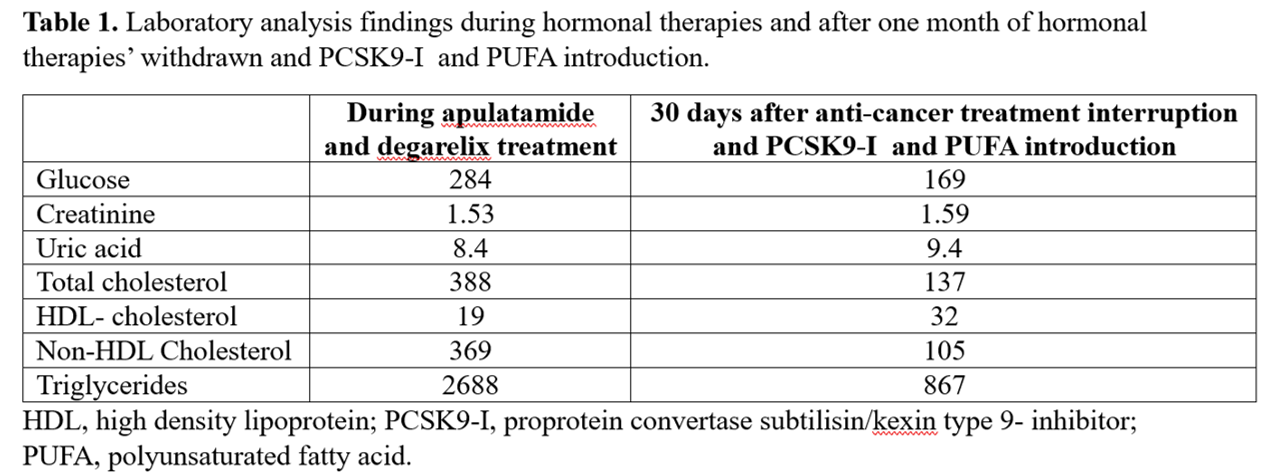
Background: Apulatamide, a nonsteroidal androgen receptor inhibitor, and degarelix, a gonadotrophin releasing hormone antagonist, are used as hormonal therapies for advanced prostate cancer (aPC) treatment. However, they may increase the risk of cardio-metabolic diseases which are the main cause of non-cancer-related death in patients with PC. We report a clinical case of a patient with aPC treated with apulatamide and degarelix who had severe hypertriglyceridemia after a few months of treatment. Case Report: A 76–year–old man with a history of type 2 diabetes, managed with insulin therapy, and multidistrict atherosclerotic disease (previous percutaneous coronary artery (PCI) revascularization, coronary artery bypass graft surgery, and peripheral artery disease, with last PCI performed three years before) presented for a follow-up out-patient visit. His laboratory analyses showed severe dyslipidemia (table 1) even though he was treated with high-intensity statin and ezetimibe for years. In the patient’s clinical history there was a recent diagnosis of aPC treated with apulatamide and degarelix for about 3 months. Although laboratory analyses before starting cancer treatment were not available, the patient reported annual lipid level checks with values in the “normal range”. After consultation with the oncologist, the treatment with apulatamide and degarelix was withdrawn and dyslipidemia treatment was optimized by adding evolocumab 300 mg once a month and a mixture of omega 3 fatty acid (1 g three times a day). Insulin dosages were increased and gliflozin treatment was started. At the lipid profile assessment a month later, total cholesterol levels were reduced by 65%, non-HDL cholesterol by 72%, and triglycerides by 68%. Glycemic control also improved, although, as lipid parameters, it was still not optimal (table 2). Liver and pancreatic enzymes were found in the normal range. A further check of lipid levels has been scheduled one month later but the results are not yet available. Conclusions: Hormonal therapies are the cornerstone for the pharmacological systemic treatment of aPC. However, these may cause alterations in lipid levels and glucose metabolism which can accelerate atherosclerosis and promote thrombotic events. Our case shows how the withdrawn of hormonal therapies together with the starting of powerful lipid-lowering agents may allow to improve lipid and glycemic profile and reduce atherosclerotic cardiovascular risk.