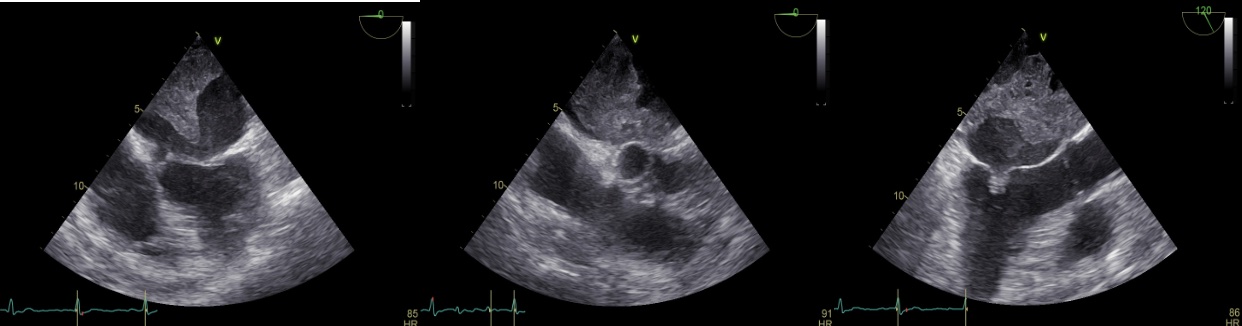
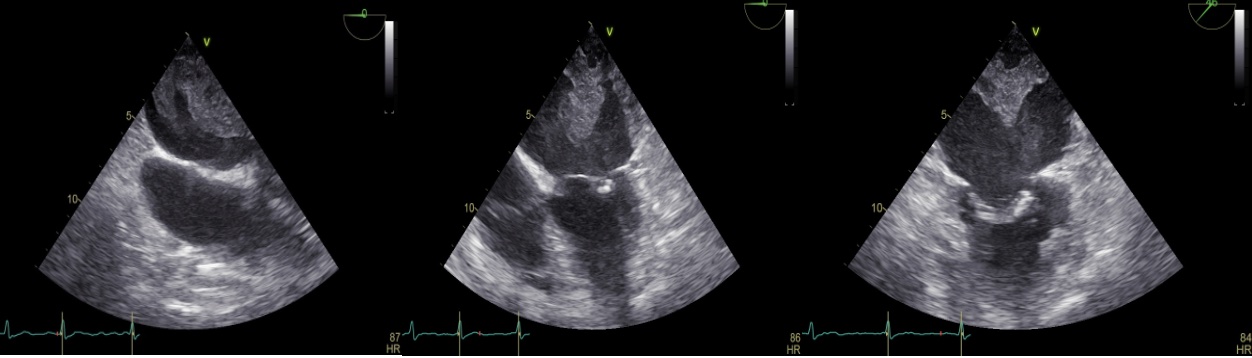
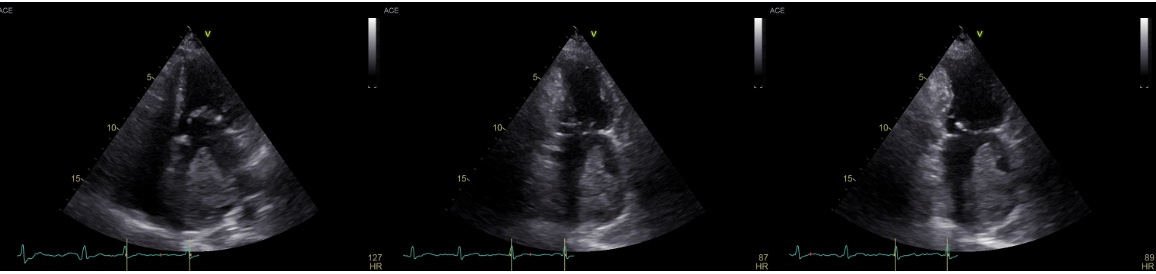
Introduction. Giant left atrial (LA) thrombi are rare but life-threatening complications of valvular atrial fibrillation. Diagnosis may be challenging in complex clinical settings and management remains controversial. We report a case of massive LA thrombosis complicating rheumatic mitral stenosis, subtherapeutic anticoagulation and sepsis. Case Report. A 63-year-old Albanian woman, with a complete language barrier and a history of rheumatic mitral stenosis, permanent atrial fibrillation on vitamin K antagonists, prior ischemic stroke and peripheral arterial disease, was initially hospitalized for non-revascularizable critical limb ischemia. Two weeks later, she was readmitted with fever and acute cognitive impairment. Laboratory tests showed leukocytosis, elevated C-reactive protein, and subtherapeutic anticoagulation (INR 1.2). Empiric broad-spectrum antibiotics and low-molecular-weight heparin were initiated. Transthoracic echocardiography revealed severe LA dilatation with a large hyperechoic mass; due to suboptimal imaging, transesophageal echocardiography (TEE) was performed. TEE demonstrated a sessile, homogeneous mass occupying over 60% of the LA cavity, with complete occlusion of the left atrial appendage, consistent with a giant thrombus. Marked spontaneous echo contrast was present. The mitral valve was calcified and thickened, causing moderate stenosis (mitral valve area 1.2 cmq). Blood cultures grew Staphylococcus aureus and urine cultures isolated ESBL-producing Escherichia coli ; targeted antibiotic therapy and optimized anticoagulation were instituted. Despite treatment, the patient developed septic shock and multiorgan failure with fatal outcome. Discussion. Giant LA thrombosis results from the interaction between atrial fibrillation–related blood stasis, rheumatic valve disease, inadequate anticoagulation and systemic inflammation. In this setting, TEE is crucial for defining thrombus burden when transthoracic imaging is limited. Although anticoagulation is the cornerstone of therapy, surgical thrombectomy may be considered in selected cases; however, severe instability and active infection may preclude invasive strategies. Conclusion. This case underscores the dramatic course of giant LA thrombosis in high-risk valvular atrial fibrillation and highlights the importance of early multimodality imaging and individualized therapeutic decision-making in critically ill patients.