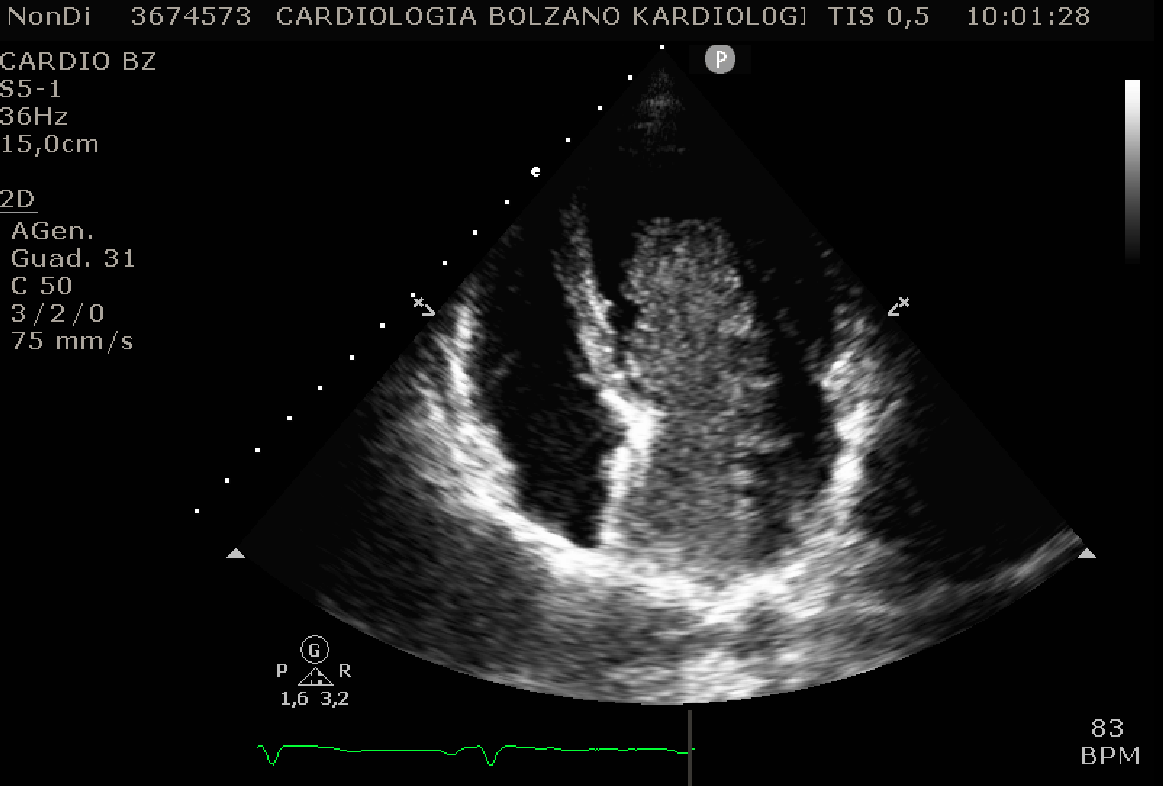
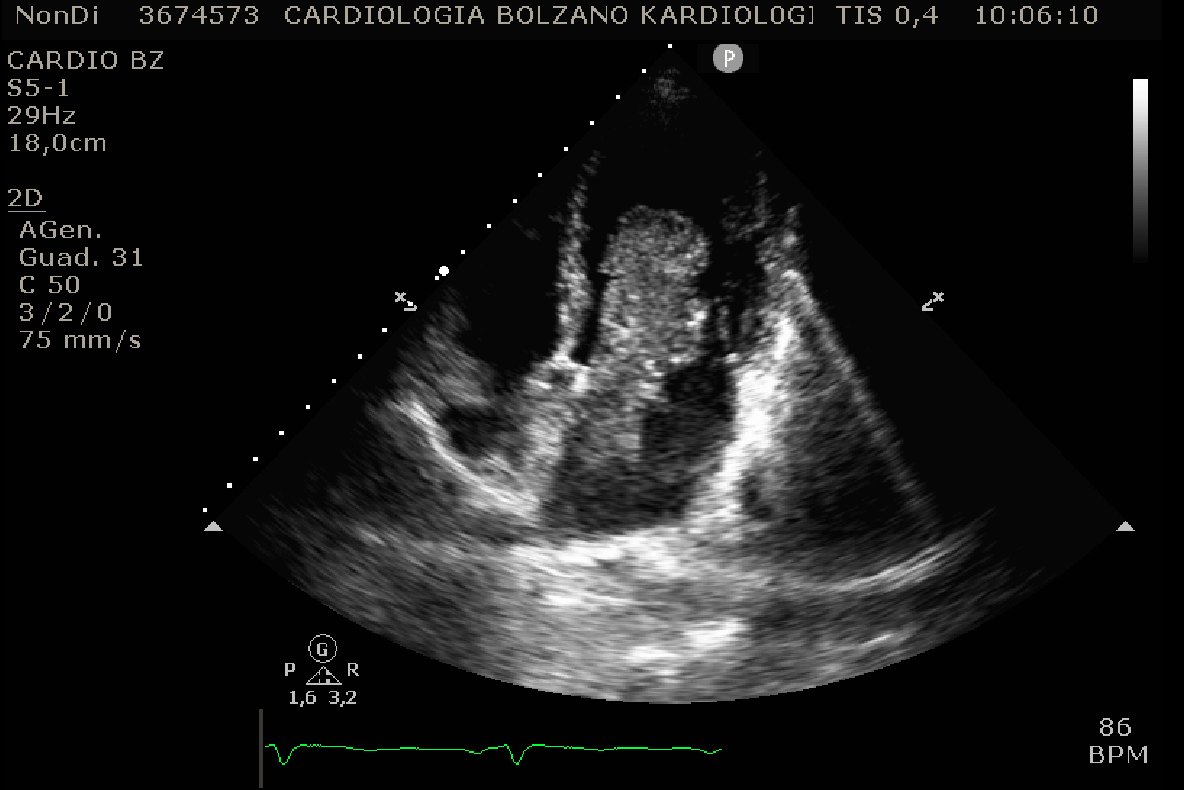
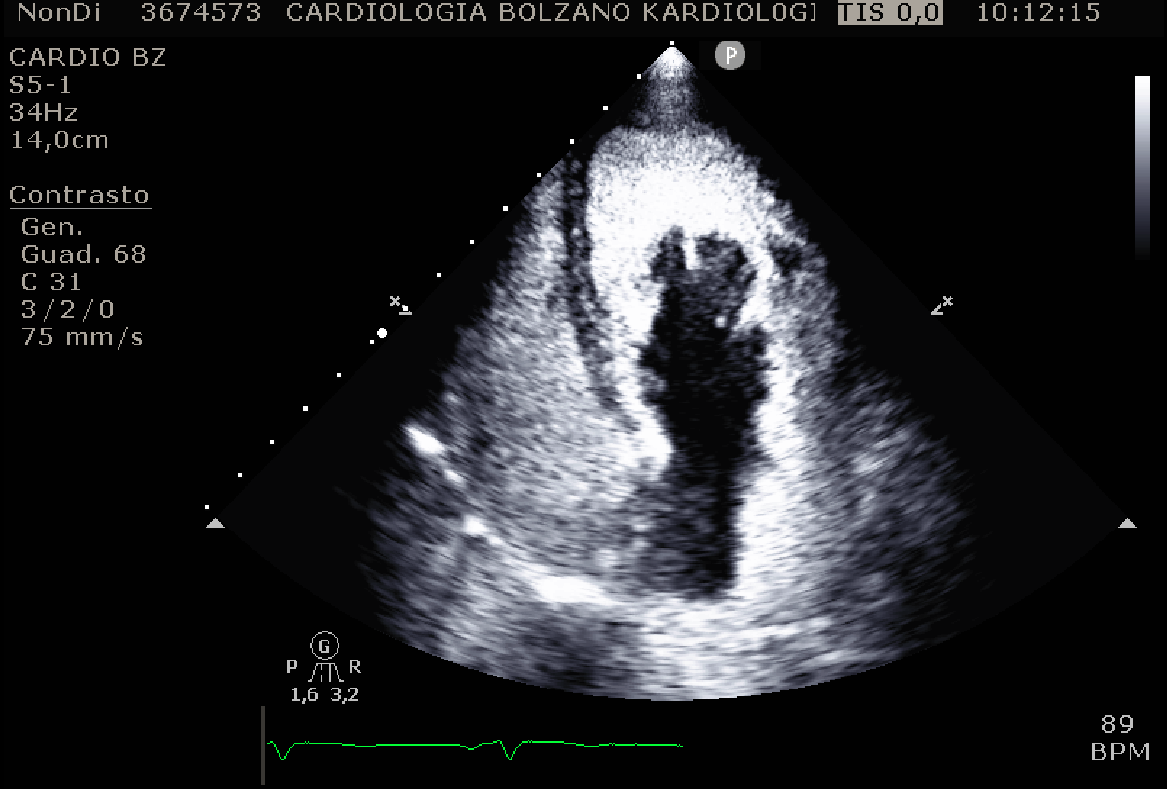
A 65-year-old woman. Past medical history essentially unremarkable. No home medications. On the morning of 26/11/2025, at around 10:00 a.m., while at work, she developed a sudden motor deficit of the right upper limb and a speech disturbance. Emergency services (112) were alerted for urgent transport (airlifted) to our Emergency Department (ED). The patient arrived at the ED at 11:00 a.m. On medical examination, she was alert, afebrile, hemodynamically stable (BP 140/95 mmHg), with moderate aphasia and mild hypoesthesia of the right hemibody. The ECG showed sinus rhythm without significant ST-T abnormalities. Complete blood count, liver and kidney function tests, blood sugar, PT and aPTT were within normal limits. Neurological assessment revealed an NIHSS score of 13. The patient was urgently taken to Radiology for a brain CT and CT angiography of the extra- and intracranial vessels. On initial radiological evaluation, no significant acute ischemic or hemorrhagic lesions were detected. Therefore, at 11:30 a.m., systemic thrombolysis with Alteplase was initiated. At 11:40 a.m., the neurologist was alerted by the radiologist because a more detailed review of the images using dedicated software showed early demarcation of recent ischemic lesions in the left frontal and parieto occipital regions, as well as occlusion of the left posterior cerebral artery in the P2 segment. Thrombolysis was immediately stopped (only the 10 minute bolus had been administered), and the patient was admitted to the Stroke Unit. Over the following hours, she remained hemodynamically stable, though mild aphasia and slight clumsiness on cerebellar testing persisted. On the morning of 27/11/2025, the consulting cardiologist performed a transthoracic echocardiogram, which revealed a large intracavitary mass (maximum dimensions 8×4 cm) with a likely thin attachment to the posterior wall of the left atrium, highly mobile, with marked systolic–diastolic excursion, occupying almost the entire left atrium in systole and much of the left ventricle in diastole (see figures). The designated cardiac surgery was therefore alerted, and urgent transfer was arranged for surgical excision of the mass. The mass was successfully removed, without intraoperative or extraoperative complications . The subsequent histological examination confirmed the clinical suspicion of atrial myxoma (despite an implantation base that was atypical compared to the usual).