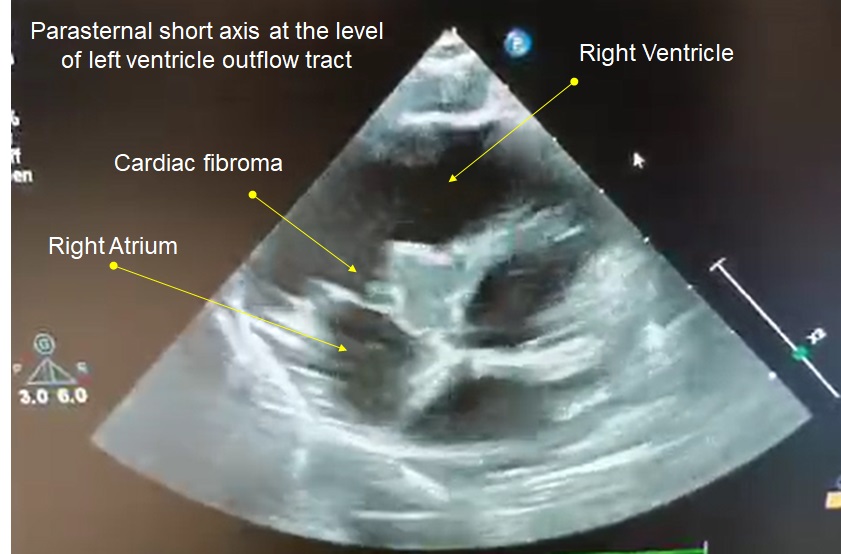
Background Cardiac fibroma (CF) is a rare benign tumors, accounting for approximately 0.5-1% of all cardiac tumors. It is more frequently observed in children and can manifest with flow obstruction, heart failure, and rhythm disturbances. CF can cause a variety of complications depending on size and location. Atrioventricular (AV) block, a dreadful complication, may require urgent surgical intervention. We describe a unique case of a child presenting with AV block secondary to interventricular septum CF. Case Presentation A previously healthy 12-month-old male was admitted to a local emergency department after a brief episode of loss of consciousness during a febrile illness. On admission the child appeared clinically stable. Physical examination was unremarkable except for the presence of age related bradycardia (70 beats per minute). An electrocardiogram revealed a 2:1 AV block that mandates his transfer to a specialized pediatric cardiology unit. Transthoracic echocardiography showed normal anatomy and normal biventricular function but revealed the presence of a large (approximately 1 cm in diameter), homogeneous, and iso-echogenic mass located on the proximal interventricular septum, nearly beneath the tricuspid valve. The lesion was not responsible of obstruction in the right ventricular inflow or outflow. The ultrasound anatomy of the lesion and the clinical context suggested primary CF. Oncologic screening excluded the presence of metastatic tumor. A cardiac magnetic resonance confirmed the clinical suspicion. Although clinically stable, the patient developed paroxismal episodes of third-degree AV block that mandates epicardial pacemaker implantation. Discussion Interventricular septal CF are a rare form of cardiac tumor in children. While typically benign, its clinical implications depend on its size and position. In this case, the CF was located in a critical area of the cardiac conduction system, leading to progressive AV block. AV blocks associated with cardiac fibromas are rare but can be life-threatening due to the risk of complete heart block and sudden cardiac arrest. Urgent multidisciplinary evaluation is essential for such cases to determine the optimal management, which may include close monitoring, antiarrhythmic therapy, or surgical resection of the tumor. In cases where the tumor is inaccessible or surgery carries high risks, pacemaker implantation may be necessary to prevent catastrophic outcomes.