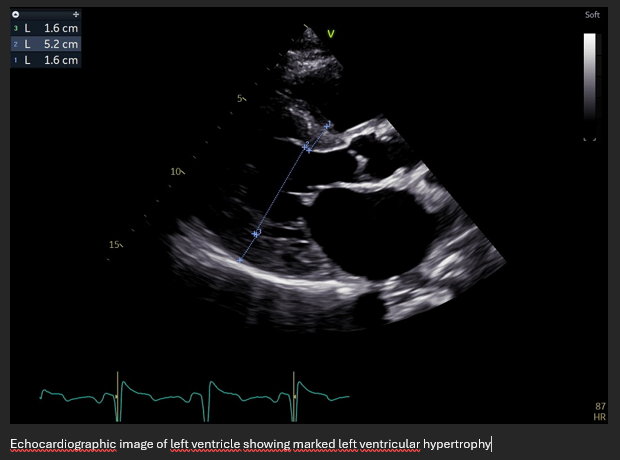
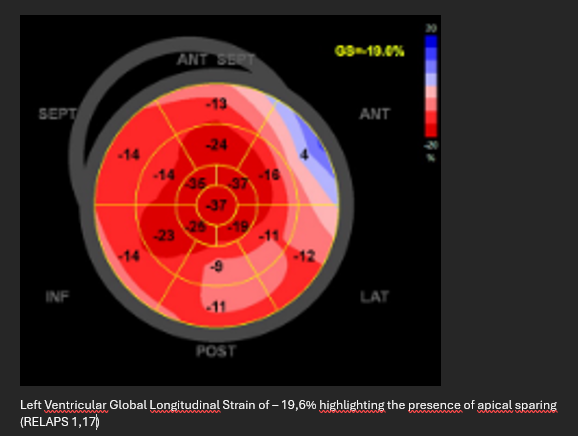
BACKGROUND : Transthyretin amyloidosis is caused by extracellular deposition of misfolded transthyretin protein and may involve the heart, leading to heart failure and arrhythmias. ATTR can be wild-type or hereditary (variant ATTR). One of the pathogenic variants is Val122Ile, prevalent in individuals of West African ancestry. Non-invasive diagnosis of ATTR cardiomyopathy relies on bone scintigraphy combined with exclusion of monoclonal gammopathy. However, discordant clinical and imaging findings may occur, particularly in pluricomorbid patients. CASE PRESENTATION: A 49-year-old Nigerian man with multiple cardiovascular risk factors, long-standing diabetes mellitus, end-stage chronic kidney disease on dialysis, and advanced peripheral arterial disease with lower limb amputation was evaluated for heart failure. NT-proBNP was 2574 pg/mL and troponin 265 ng/L. Echocardiography showed left ventricular hypertrophy, reduced systolic function (LVEF 35–40%), severe mitral and tricuspid regurgitation and biatrial enlargement. Coronary CT angiography revealed a moderate plaque burden with minimal mid left anterior descending artery stenosis. Absence of opacification of the posterior interventricular branch was reported, of uncertain significance. Cardiac magnetic resonance demonstrated left ventricular hypertrophy with moderate systolic dysfunction and a non-ischemic late gadolinium enhancement pattern; T1 and T2 mapping were not assessable. Serum and urine immunofixation were negative. Bone scintigraphy showed Perugini 0, while genetic testing identified a pathogenic TTR p.Val142Ile mutation. Although a Perugini score of 0 precludes non-invasive diagnosis of ATTR-CM, it does not fully exclude the disease in patients with high pre-test probability. Moreover, chronic dialysis raises the possibility of alternative or concomitant forms of amyloidosis not detectable by bone scintigraphy. CONCLUSIONS: This case highlights the limitations of current non-invasive diagnostic algorithms for cardiac amyloidosis and the need for an integrated, individualized approach, especially in highly pluricomorbid patients. In such settings, cardiac manifestations may reflect an overlap of different pathological processes complicating both diagnosis and management. Moewove, severe renal impairment may limit access to disease-modifying therapies for hereditary ATTR. Personalized clinical decision-making beyond standardized diagnostic pathways is therefore essential in real-world patients