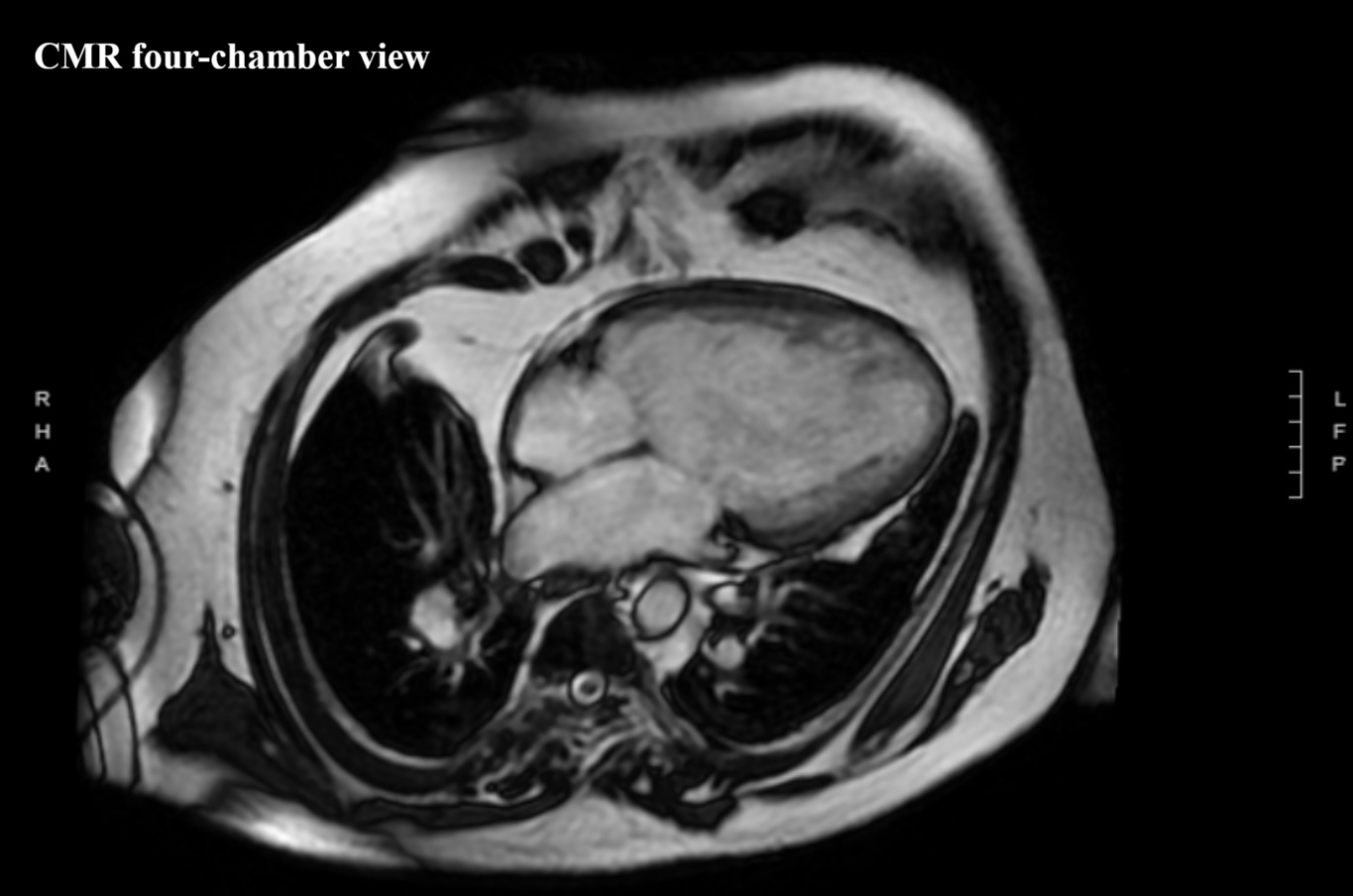
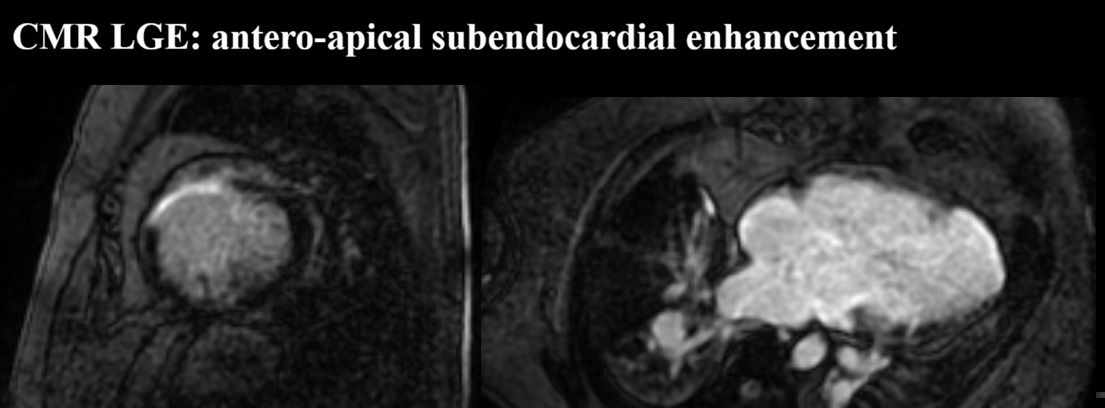
We report a 61-year-old man with unrepaired single-ventricle physiology (double inlet left ventricle, mesocardia, malposed great vessels) and stable chronic cyanosis (baseline SpO2 80–85%). In the absence of a “protective” pulmonary stenosis, lifelong high pulmonary flow and pressure led to pulmonary vascular remodeling and increased resistance, resulting in severe pulmonary arterial hypertension (PAH) with Eisenmenger-type physiology; the single ventricular pump is highly preload-, cardiac rhythm-, and systemic pressure–dependent. The course is complicated by acquired ischemic heart disease: an anterior acute coronary syndrome in 2015 in the setting of anomalous coronaries and supply–demand mismatch. Cardiac MRI showed severe dominant-ventricle dilation, EF ~33%, and antero-apical subendocardial late gadolinium enhancement. Right-heart catheterization confirmed severe PAH with PAP 120/22 mmHg (mean 55), PAWP 9 mmHg and PVR 6.2 WU, supporting initiation of triple PAH therapy (macitentan, sildenafil, selexipag) with close monitoring of systemic pressure and volume status. Clinical decompensations were triggered by atrial fibrillation or atrial tachycardia with high ventricular response, managed with rhythm and/or rate control (amiodarone, digoxin, cautious beta-blocker titration) and tailored decongestion. Non-invasive ventilation with positive pressures (BiLevel) was set conservatively given the effects of intrathoracic pressure on venous return and pulmonary circulation. Long survivors with DILV in natural history are exceedingly rare and appear to cluster into two phenotypes: “balanced” circulations with restricted pulmonary flow, and exceptional cases without protection who develop pulmonary vasculopathy. This patient belongs to the latter and is notable for triple PAH therapy; depressed systolic function may have mitigated pulmonary flow overload, contributing to a fragile equilibrium. Arrhythmic/sudden-death risk stratification in a single ventricle with scar led to ICD counselling, which the patient refused. Unrepaired DILV reaching the sixth decade with severe PAH is exceptional; management should remain physiology-driven.