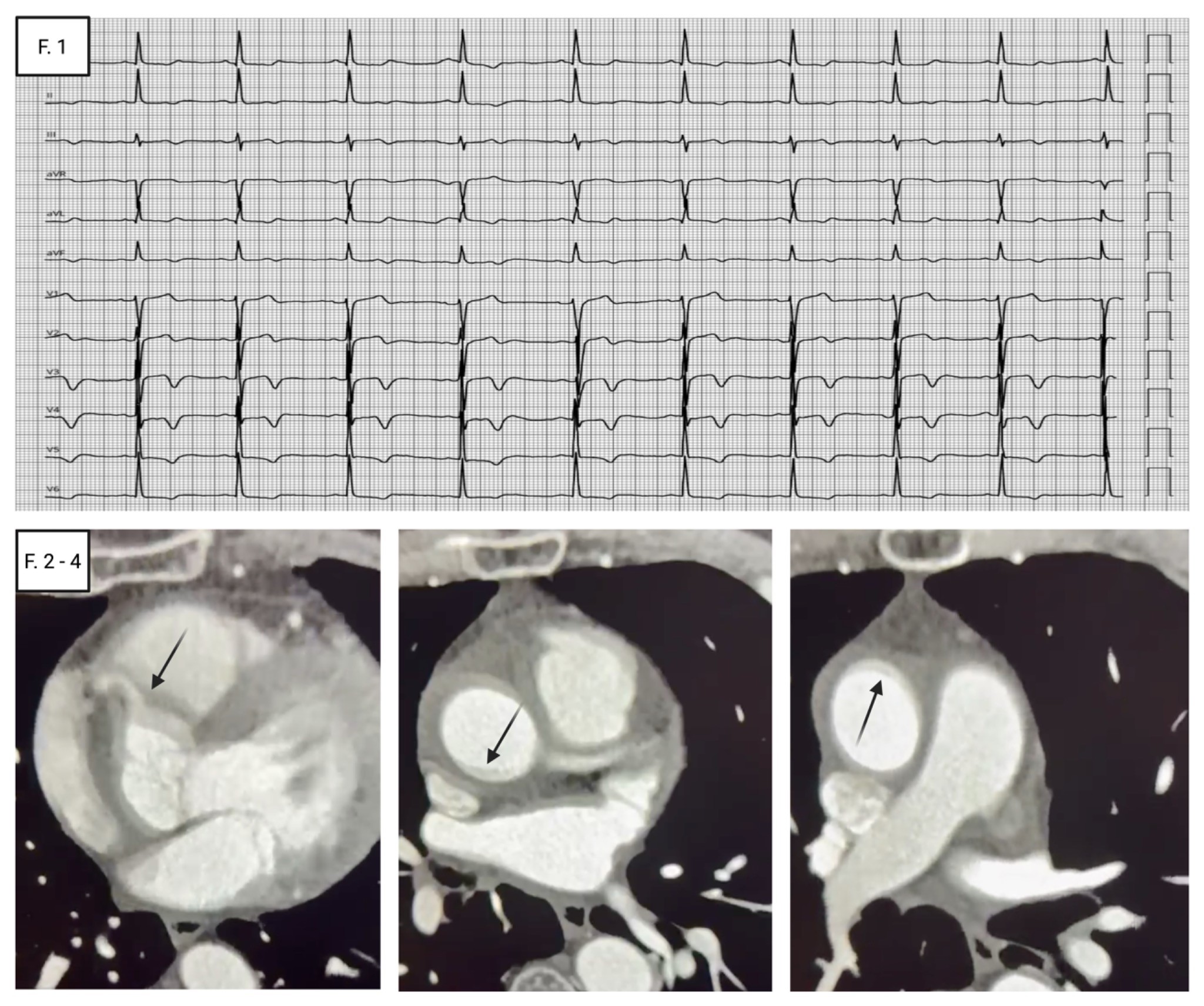
A 67-year-old man presented to the ED with acute radiating chest pain. He was haemodynamically stable but unresponsive to intravenous nitrates. The ECG showed an ACS-like pattern with persistent T-wave inversion in the inferior and V3–V4 leads, biphasic T waves in the lateral leads, resembling a Wellens type A–like pattern (Fig. 1). Biomarkers were discordant: high-sensitivity troponin was negative, D-dimer was at the upper reference limit. Urgent transthoracic echocardiography demonstrated a non-dilated left ventricle with mildly reduced systolic function and regional hypokinesia of the basal interventricular septum and inferior wall. The aortic root and ascending aorta were dilated (50 mm; 28 mm/m²), in the setting of a tricuspid aortic valve with mild-to-moderate aortic regurgitation. Focal aortic wall thickening/lamination raised suspicion of acute aortic syndrome, with a small pericardial effusion. Computed tomography angiography confirmed a crescentic hyperattenuating mural thickening (10 mm) along the right lateral ascending aorta and aortic arch, consistent with type A intramural haematoma with right coronary ostial involvement and haemopericardium (Fig. 2-4). The patient was transferred to a tertiary aortic centre for high-risk features. He underwent urgent open repair with ascending aortic resection and replacement using a 30-mm Gelweave graft. The postoperative course was uneventful. Predischarge TTE showed mildly reduced LV systolic function with persistent inferior wall hypokinesia, and the patient was discharged on postoperative day 9 to cardiac rehabilitation. Acute aortic syndromes (AAS) are the “great mimickers”. IMH, accounting for approximately 5–25% of AAS, reflects haemorrhage within the aortic media. Type A IMH may mimic ACS and, albeit rarely, present as STEMI when compromises a coronary ostium (most often the right coronary artery). Presentation mimicking a Wellens type A pattern classically linked to critical proximal LAD occlusion (OMI), is exceptional and increases the risk of diagnostic anchoring. Because outcomes are profoundly time dependent—particularly with coronary or cerebral malperfusion—misdiagnosis may be catastrophic, and an ACS-driven pathway (urgent angiography and antithrombotic escalation) may be hazardous. This case supports a deliberate bedside “rule-out” strategy for acute aortic syndrome in ED chest-pain pathways, expecially with discordant clinical or laboratoristic findigs.