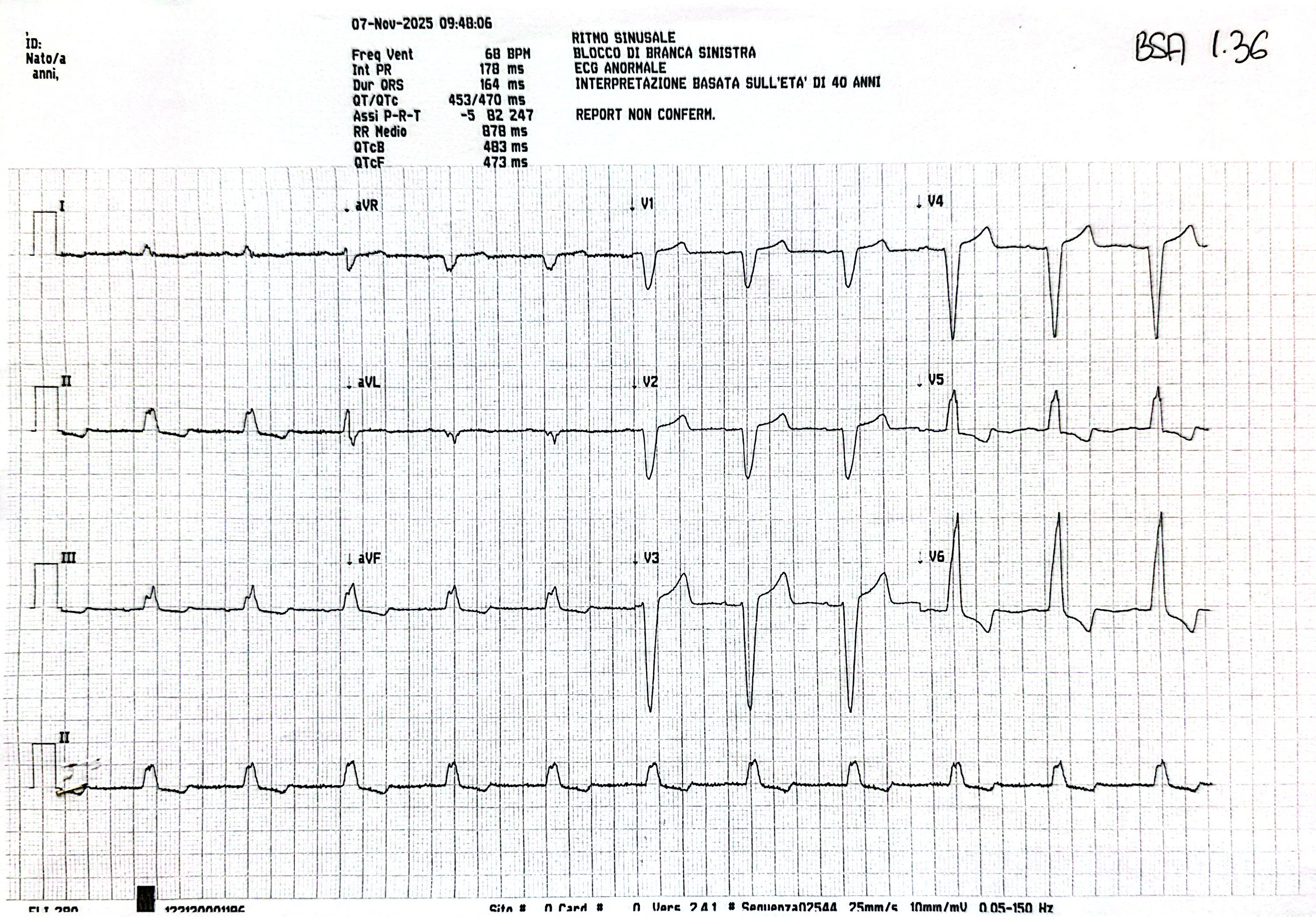
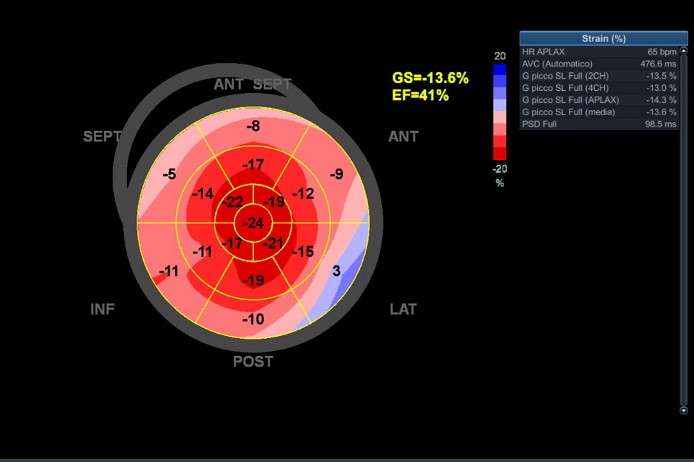
A 64-year-old woman with a history of arterial hypertension, type 2 diabetes mellitus and end-stage chronic kidney disease on hemodialysis, who was admitted to our hospital for acute heart failure. At admission the patient was hemodynamically stable with signs of central and peripheral congestion. Electrocardiography showed sinus rhythm with left bundle branch block and secondary ventricular repolarization abnormalities. Transthoracic echocardiography revealed eccentric left ventricular hypertrophy with severely reduced left ventricular ejection fraction (LVEF 33%). Coronary angiography excluded significant coronary artery disease. Cardiac magnetic resonance (CMR) demonstrated meso-subendocardial late gadolinium enhancement (LGE) in the basal inferolateral wall, associated with diffuse elevation of native T1 values and extracellular volume (ECV), findings consistent with infiltrative cardiomyopathy. Given the suspicion of cardiac amyloidosis, a peri-umbilical fat pad biopsy was performed and the patient was discharged in relatively good conditions. One month later, she was readmitted due to central venous catheter (CVC) dysfunction caused by extensive central venous thrombosis, requiring catheter removal, percutaneous transluminal angioplasty with stent implantation in the superior vena cava, and subsequent CVC repositioning. Histological examination confirmed the presence of serum amyloid A (SAA) deposits in the periumbilical fat tissue. Follow-up echocardiography showed stable findings with LVEF equal to 33% with markedly reduced global longitudinal strain and a relative apical sparing pattern. Conclusions. Cardiac involvement in AA amyloidosis is rare and typically described in advanced stages of the disease. In our patient, the clinical history was dominated by renal failure of unknown origin, which rapidly progressed to end-stage renal disease requiring hemodialysis. The cardiac presentation occurred six years after dialysis initiation and became evident in the absence of a previously recognized inflammatory disease. The underlying inflammatory disorder is still under investigation, and the lack of an early etiological diagnosis likely delayed recognition of SAA amyloidosis. In this clinical context, advanced echocardiography and CMR played a pivotal role in the detection and characterization of cardiac involvement; most importantly, comprehensive cardiac phenotyping led to the diagnosis of a previously unrecognized systemic disease.