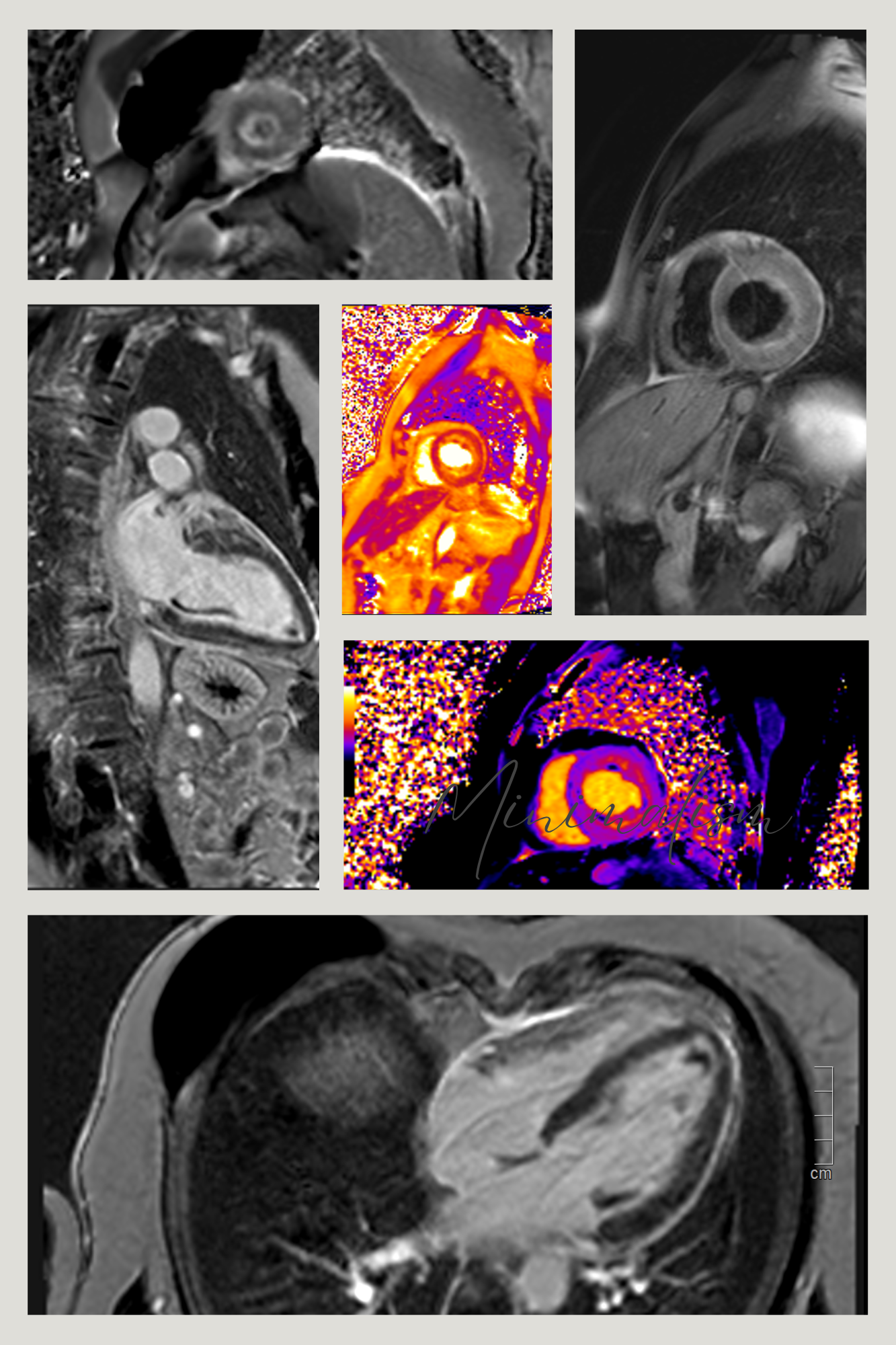
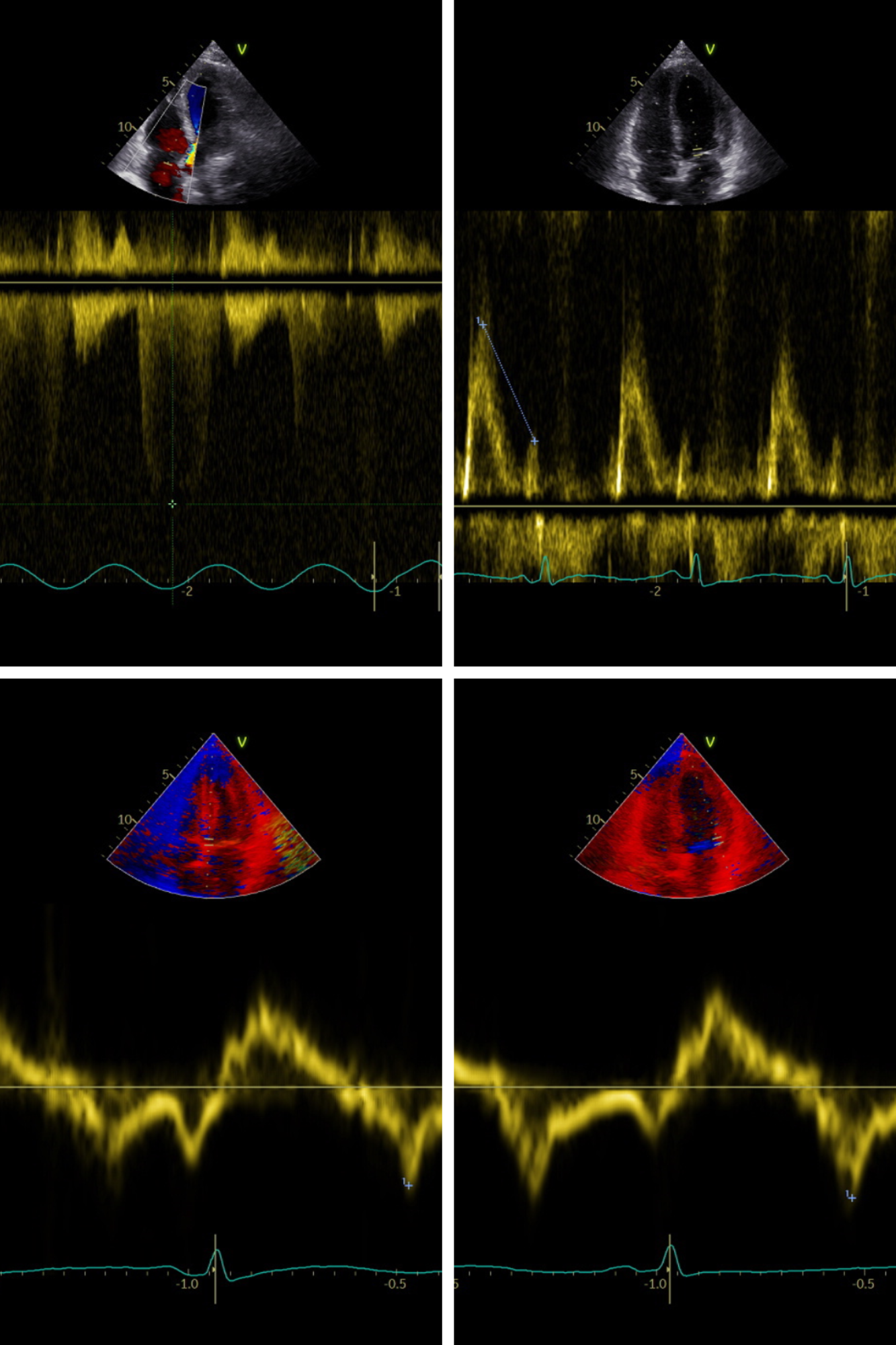
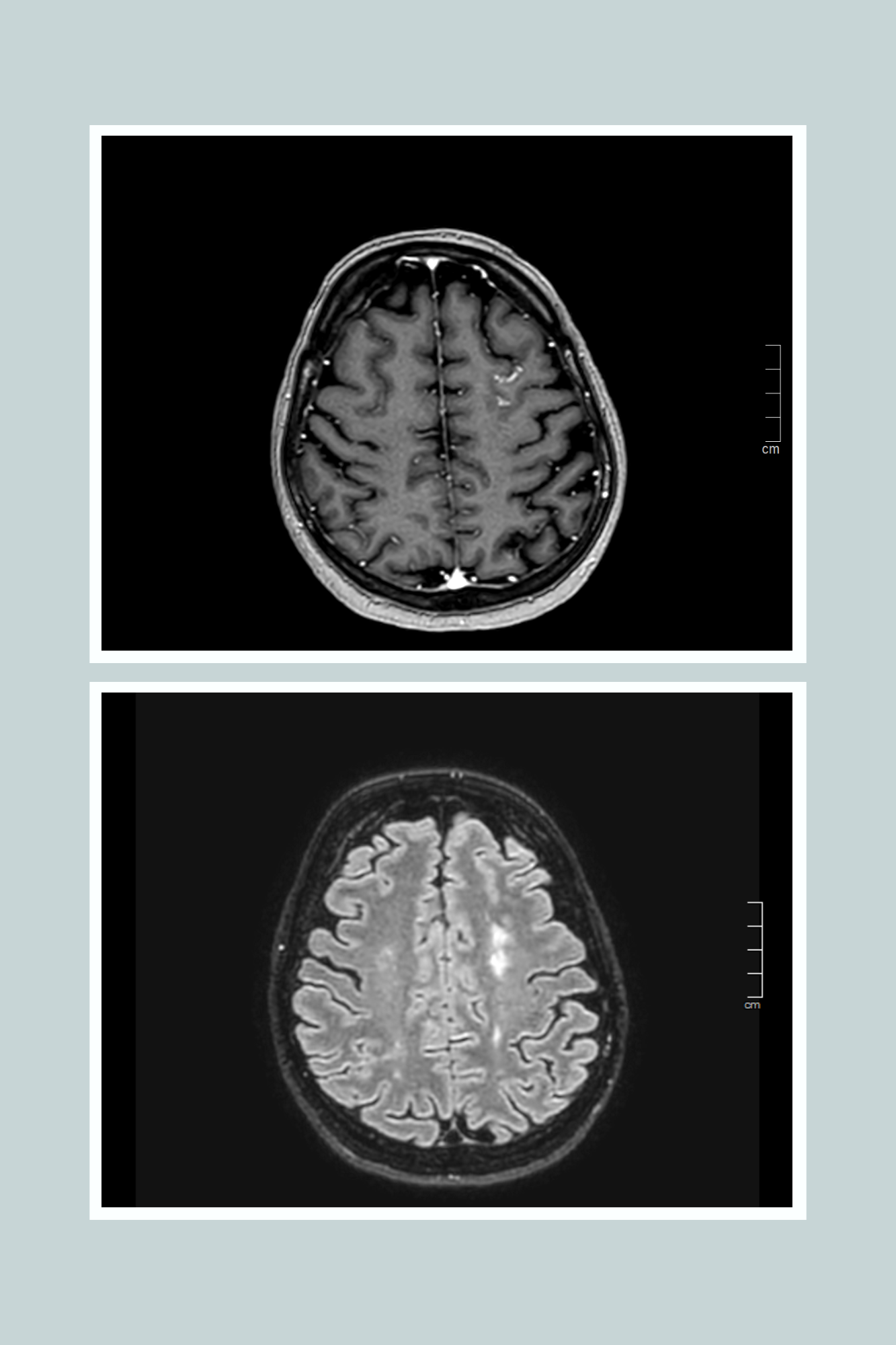
A 61-year-old woman presented to the emergency department with dyspnea and chest pain radiating to the back at rest. Laboratory tests showed creatinine 1.76 mg/dL, stable hsTnT elevation (264→256 pg/mL), NT-proBNP 19,090 pg/mL, and D-dimer 1,969 ng/mL. ECG revealed sinus rhythm with diffuse inferolateral ST-segment depression. Echocardiography demonstrated preserved LV systolic function (LVEF 65%), increased wall thickness with apical kissing, borderline RV function, pulmonary hypertension, and diastolic dysfunction with elevated filling pressures. Medical history included chronic kidney disease, asthma with nasal polyposis, eosinophilia, and prior mastectomy for in situ ductal carcinoma. Immunological evaluation had suggested interstitial nephropathy with possible IgG4 involvement. Given the combination of asthma, eosinophilia, and nasal polyposis, she fulfilled criteria for eosinophilic granulomatosis with polyangiitis (EGPA). CT angiography excluded pulmonary embolism but showed mosaic attenuation. Laboratory tests confirmed marked eosinophilia (2,170 ×10⁹/L, 30%) and elevated eosinophil cationic protein (216 µg/L), with further NT-proBNP increase (22,535 pg/mL). Urinalysis revealed microscopic hematuria without proteinuria. Right heart catheterization demonstrated post-capillary pulmonary hypertension (PCWP 27 mmHg). Brain MRI showed multiple T2 hyperintense lesions, consistent with multifocal vasculitis. Cardiac magnetic resonance revealed diffuse endocardial late gadolinium enhancement with extensive thrombotic layering along the LV endocardium and mitral valve, consistent with Loeffler endocarditis. The hospital course was complicated by acute pulmonary edema, restrictive diastolic filling, acute-on-chronic kidney injury (peak creatinine 4.37 mg/dL), and urinary sepsis. After multidisciplinary discussion, immunosuppressive therapy with high-dose methylprednisolone, oral prednisone, and cyclophosphamide pulses was initiated, together with warfarin. Given the highly suggestive clinical, biochemical, and imaging findings and the high bleeding risk, endomyocardial biopsy was deferred. The patient improved clinically, with stable renal function (creatinine 3.5 mg/dL) and reduced NT-proBNP at discharge. At follow-up, she remained hemodynamically stable, with reduced LV wall thickness, preserved systolic function, persistent restrictive filling, and progressive GLS improvement (from −10% to −20% at six months).