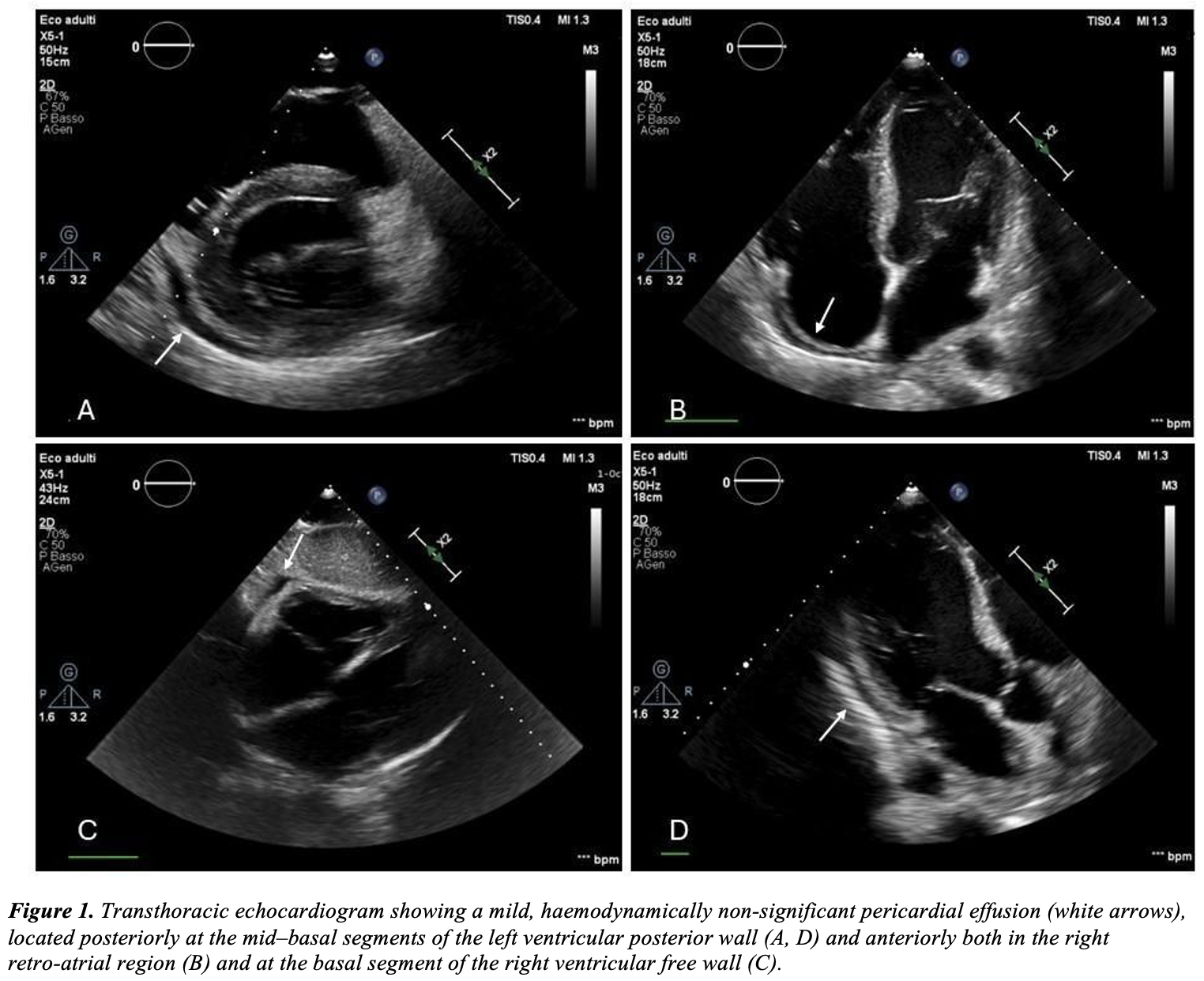
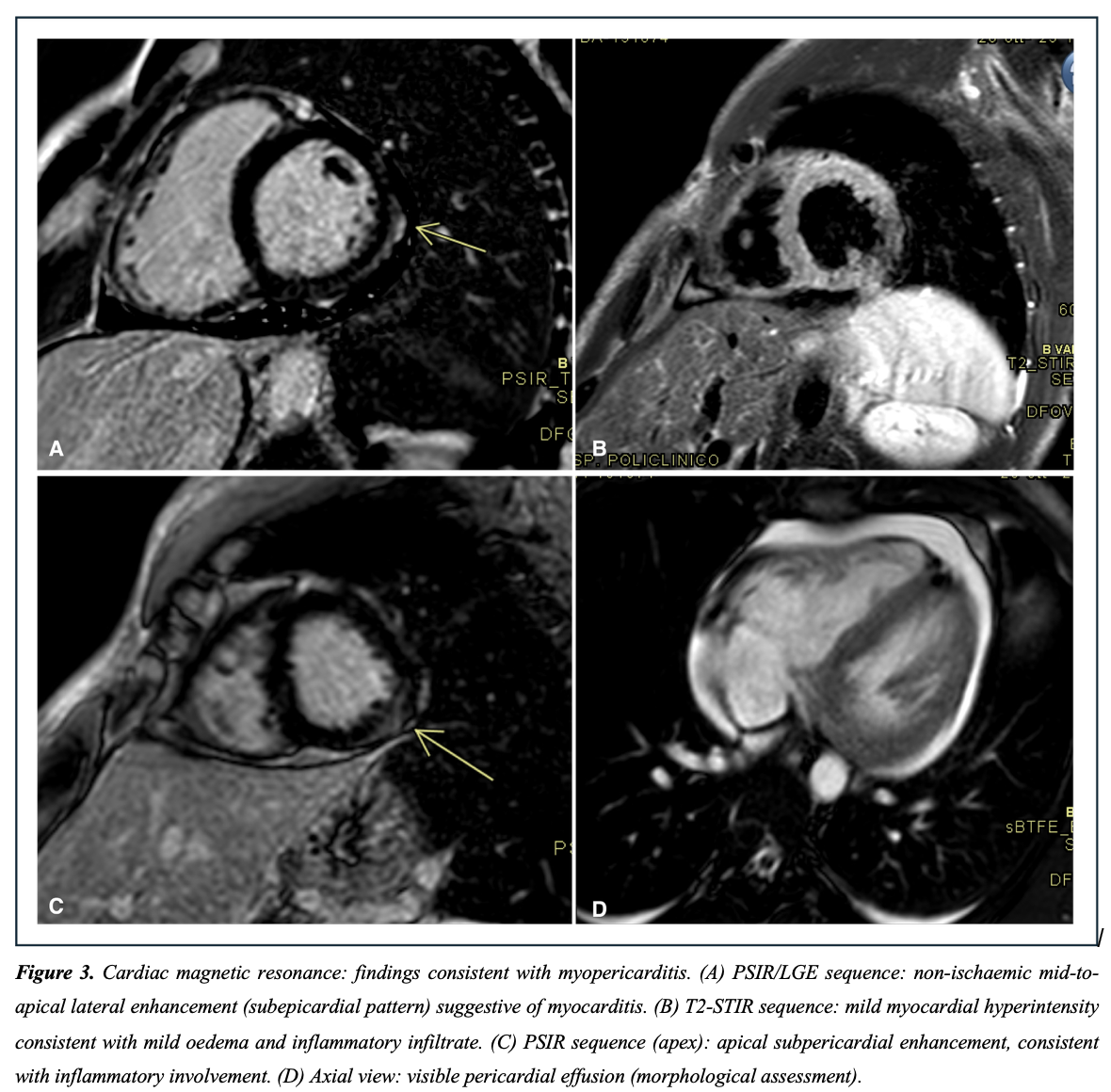
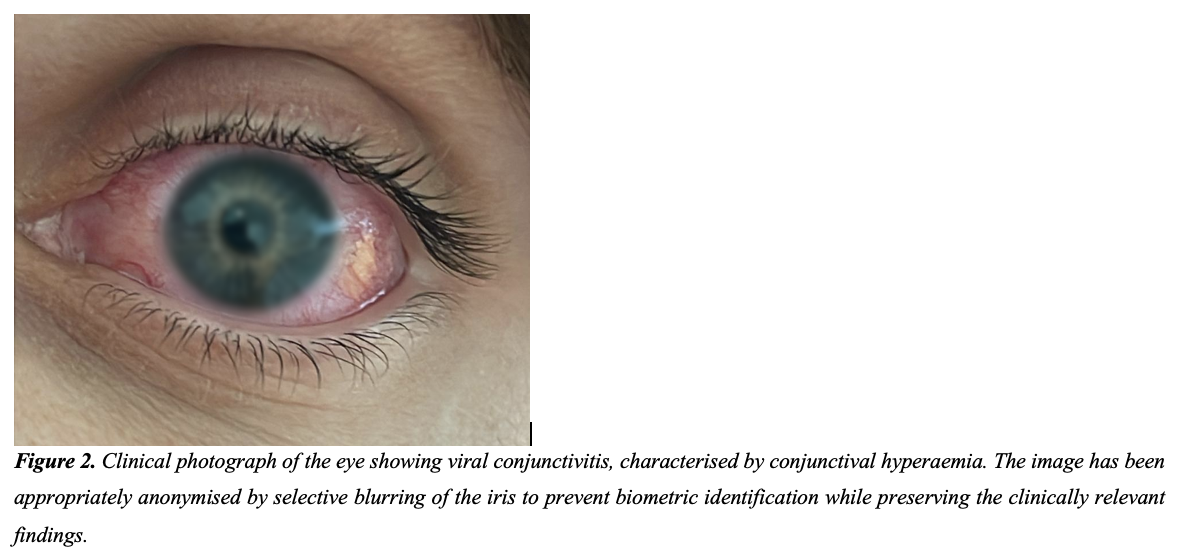
Background: Myopericarditis can be clinically “silent” and present as fever of unknown origin. In immunocompetent adults, CMV-associated cardiac involvement is uncommon and virological attribution may be uncertain. Case presentation: A 33-year-old immunocompetent, physically active man presented with 10 days of high-grade fever (up to 39.5°C), malaise, gastrointestinal symptoms and severe conjunctivitis, without chest pain, dyspnoea, syncope or palpitations. Blood tests showed intense inflammation (CRP 237 mg/L) and marked myocardial injury (hs-cTnI 3025 pg/mL) with elevated NT-proBNP (4939 pg/mL). Serial ECGs were unremarkable. Transthoracic echocardiography showed preserved left ventricular ejection fraction (~55%) and a mild pericardial effusion (max 5 mm) without haemodynamic compromise. The clinical course was stable (no major arrhythmias; downtrending troponin). Microbiological testing was negative, except for CMV IgM positivity with IgG negativity; blood CMV-DNA was undetectable, therefore no antiviral therapy was started. Treatment with ibuprofen plus colchicine and activity restriction was prescribed. Cardiac magnetic resonance was performed and confirmed subacute myopericarditis (non-ischaemic subepicardial inferolateral LGE, pericardial enhancement and effusion up to ~18 mm) with preserved biventricular function. At 4-week follow-up, symptoms and biomarkers normalised and pericardial effusion resolved. Conclusions: Persistent fever with conjunctivitis and troponin rise may conceal myopericarditis even without chest pain. According to latest ESC guidelines, early echocardiography and CMR are pivotal for diagnosis and phenotyping. Acute serous conjunctivitis is an uncommon accompanying sign that warrants accurate evaluation. Isolated CMV IgM positivity should be interpreted as suggestive rather than definitive causation when viral DNA is negative, supporting proportionate conservative management in stable immunocompetent patients. To the best of our knowledge, this is the first reported case of acute myopericarditis and conjunctivitis in a healthy subject with serology suggestive of acute CMV infection and negative serology for other common causative agents.