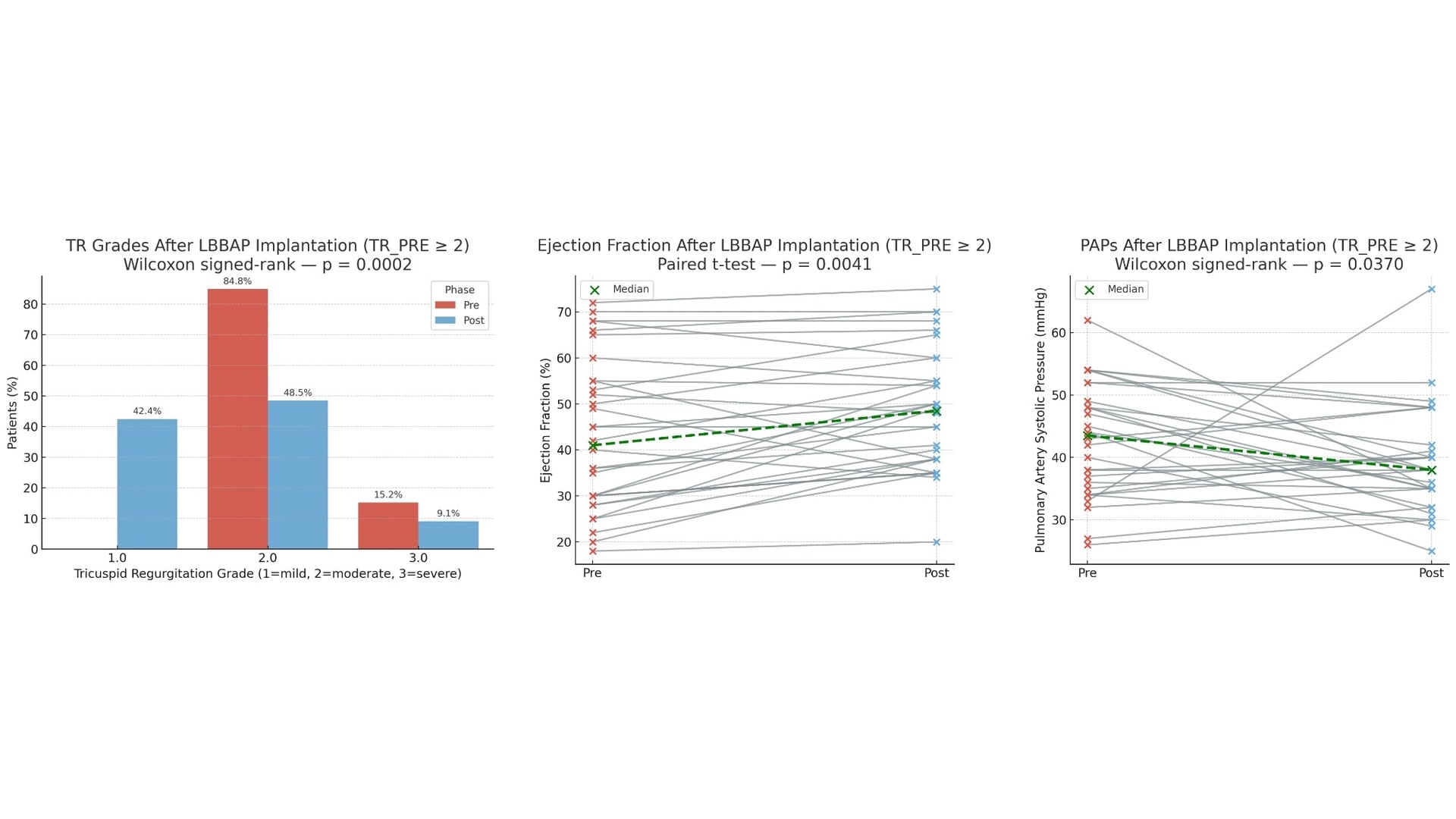
Background: Tricuspid regurgitation (TR) of moderate or greater severity is increasingly recognized as an independent predictor of adverse outcomes. Cardiac device implantation with transvenous leads has been suggested to potentially worsen TR, with reported incidences ranging from 7 to 30%. Left bundle branch area pacing (LBBAP) restores physiological ventricular activation and may offer haemodynamic advantages over traditional right ventricular pacing, potentially alleviating secondary TR. However there are limited data on the impact on worsening. Purpose: We sought to evaluate the impact of LBBAP on TR in patients presenting with clinically significant valve dysfunction. Methods: We retrospectively analyzed consecutive LBBAP patients. Patients having baseline TR less than moderate (TR < 2) and patients without complete echocardiographic follow-up were excluded. The primary endpoint was the change in TR grade. Paired analyses were performed using Wilcoxon or paired t-tests, as appropriate. Results: Of 130 patients receiving LBBAP, 50 had complete echocardiographic follow-up (median follow-up 9,5 months) and, of these, 29 (58.0%) had TR ≥ moderate at baseline and were included in the analysis. TR improved in 13/29 (44.8%), was stable in 15/29 (51.7%), and worsened in 1/29 (3.4%). The overall reduction in TR grade was statistically significant (Wilcoxon p = 0.0048). Left ventricular ejection fraction (LVEF) significantly increased from baseline (median +6.4%, p = 0.002). Estimated pulmonary artery systolic pressure (PASP) decreased (median –3.2 mmHg, p = 0.045). These changes occurred in the absence of worsening TR in any patient and were consistent across the cohort. Conclusions: In patients with moderate-to-severe TR at baseline, LBBAP was associated with a significant reduction in TR severity, together with improved left ventricular function and a favorable trend in pulmonary pressures. These findings support LBBAP as a safe pacing strategy regarding the potential worsening effect on TR and suggest it may even be protective in patients with tricuspid valve dysfunction. Confirmation in larger controlled cohorts is warranted.