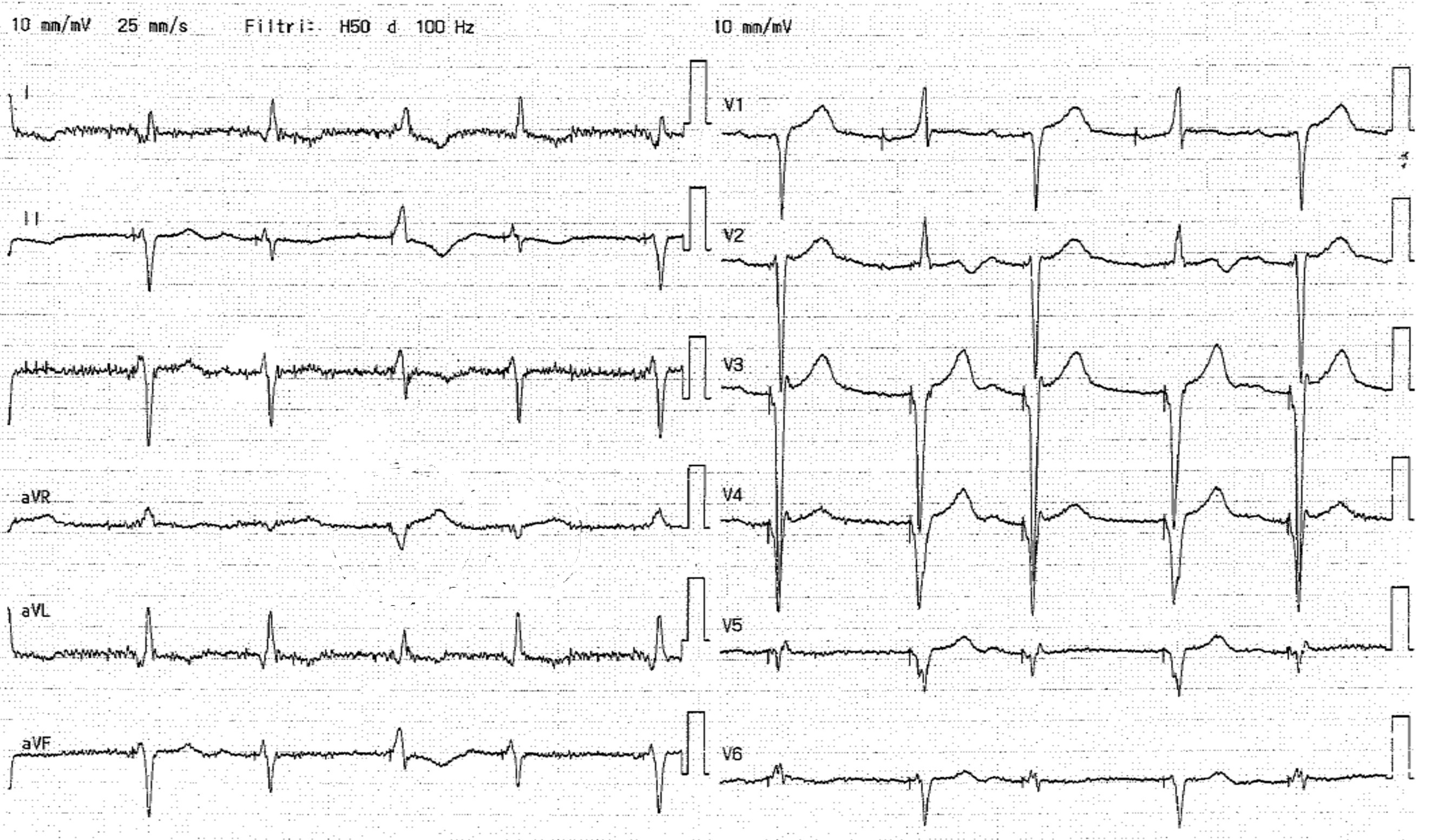
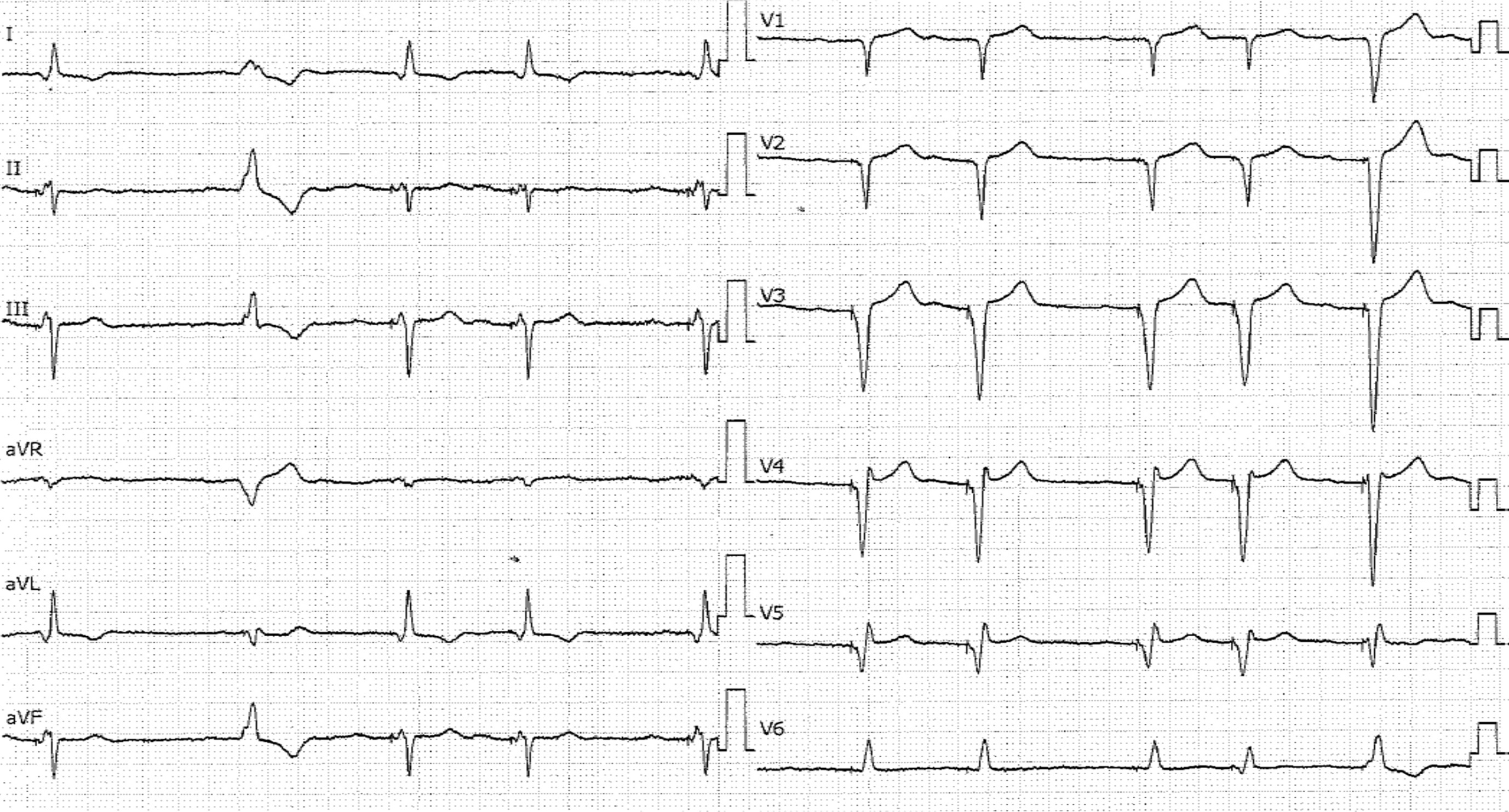
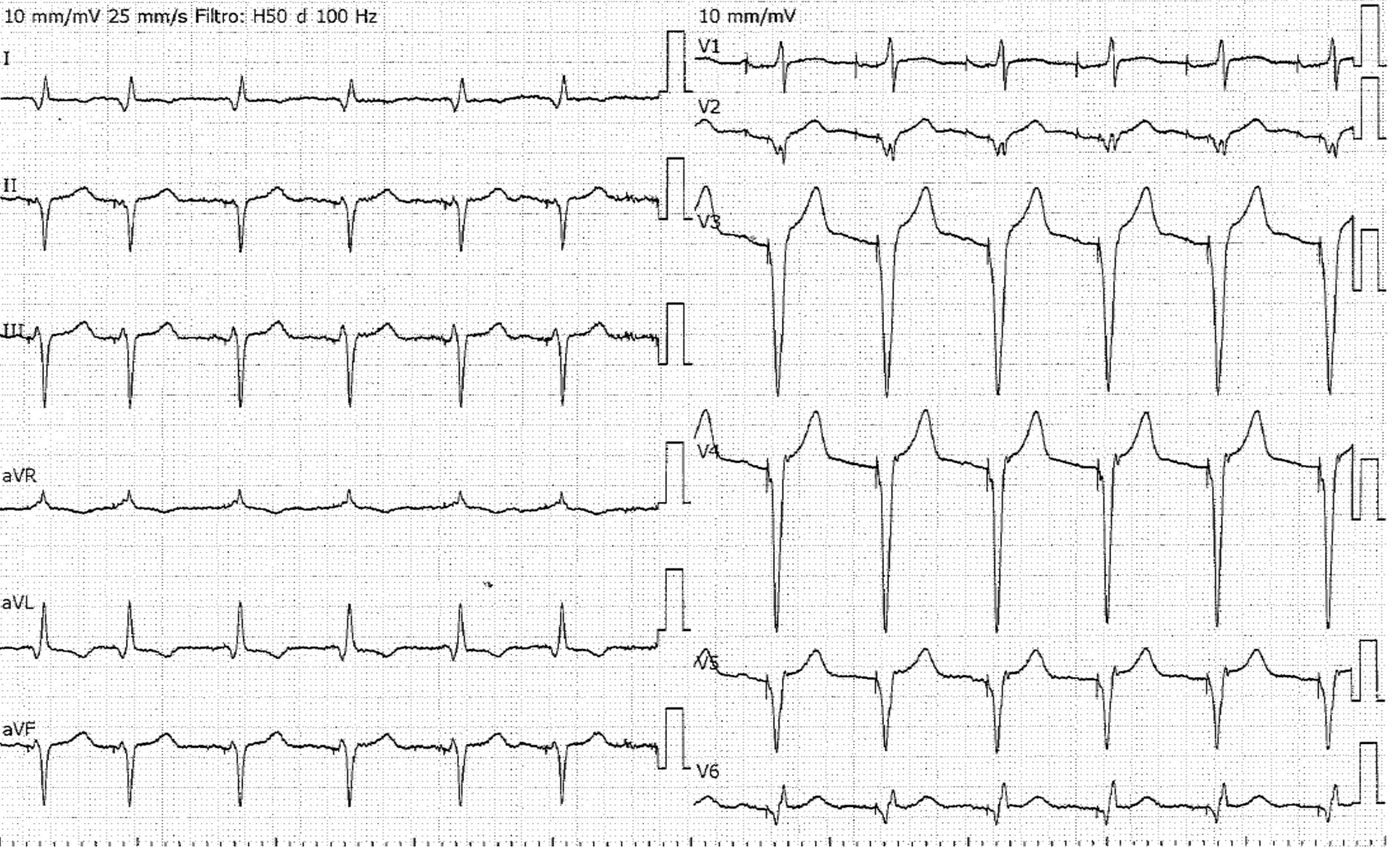
We present the case of an 85-year-old patient with hypokinetic cardiomyopathy, mitral bioprosthesis, complete LBBB on ECG. The patient underwent biventricular ICD implantation in 2013 with good clinical and echocardiographic response, without hospitalization for 10 years. He presented with an intriguing ECG: sinus rhythm with biventricular stimulation and a narrow paced QRS complex. However, the paced QRS complex, although good, varies from beat to beat depending on whether the atrium is sensed or paced (Fig 1). Specifically, the QRS complex is narrower when it follows a sensed atrium. The patient's spontaneous rhythm was sinus rhythm 55-60bpm, PQ of 200 msec, atrial ectopic beats, and a QRS complex with a LBBB morphology and a width of 160 msec. Programming the device to DDD 40 bpm we see a ventricular rhythm that was still atrial-guided and a narrow QRS complex of 100 msec, but the rhythm was disturbed by numerous ectopic beats (Fig 2).Programming the device to DDD 70 bpm with an AV delay of 150 msec we see a rhythm that was still atrial and ventricular paced, but the QRS complex appeared significantly wider, approximately 120 msec, and the tracing was regular with no ectopic beats (Fig 3). Therefore, biventricular pacing appears to be preferable when atrial depolarization is spontaneous and not electrically induced. This also corresponds to better left ventricular performance when assessed by echocardiographic perspective: longitudinal strain assessment shows better synchrony when ventricular pacing is atrial-sensed; aortic VTI is also better in this mode, especially when the AV interval is optimized. In our clinical case, we programmed the device to DDD 60/min with a 150 msec AV interval, to obtain a valid compromise between sensed and paced atrium, limiting extrasystoles, and an AV interval that favored a good ratio between E and A waves on mitral Doppler. The atrial rhythm induced by pacing (right atrial appendage) causes a delayed left atrial contraction, resulting in a reduction in diastolic ventricular filling; atrial sensing results in improved QRS fusion, which may be related to early activation of the right bundle branch simultaneous with left ventricular activation induced by left pacing. This is why the AV delay is programmed slightly longer on atrial pacing than on sensed atrial beats. This case reminds that the atrium also has a great importance in the response to cardiac resynchronization therapy.