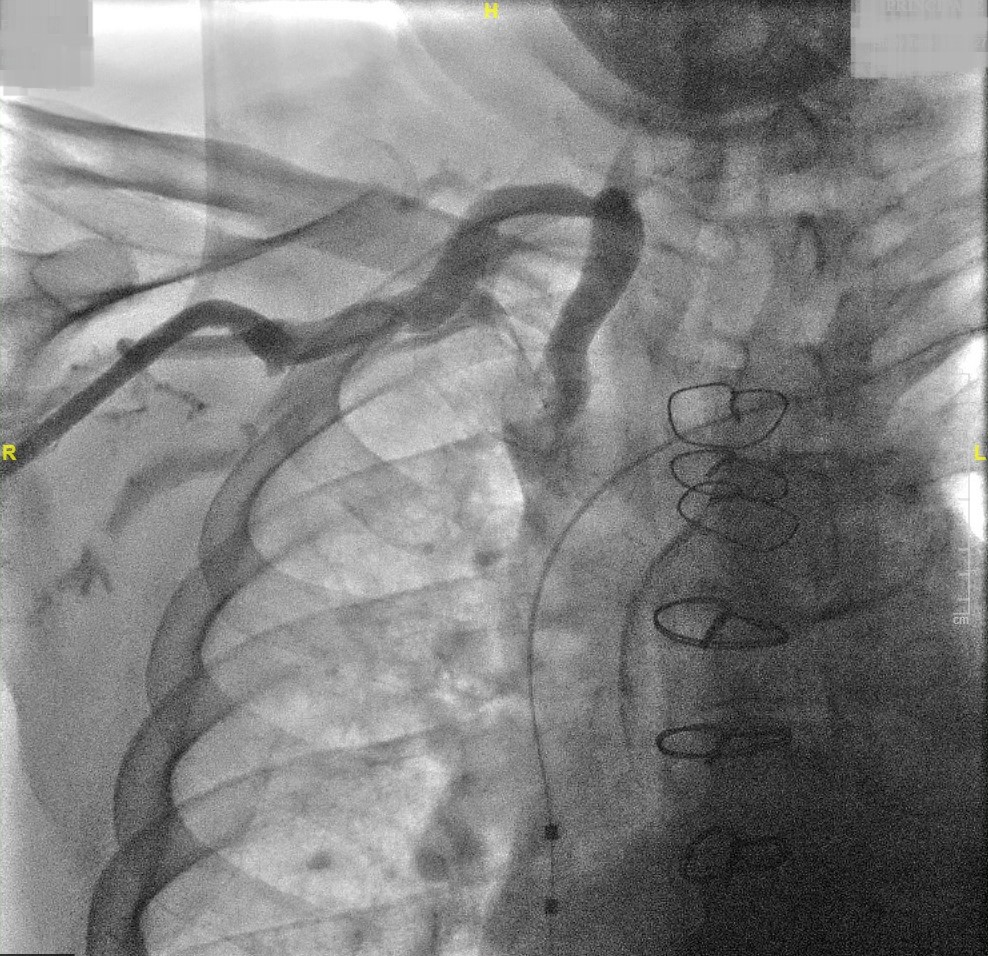
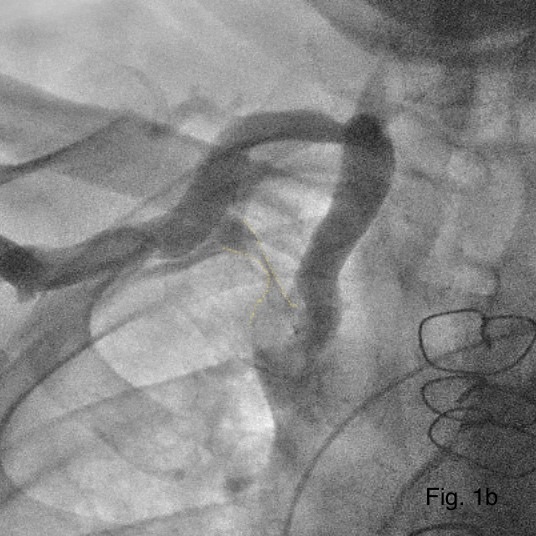
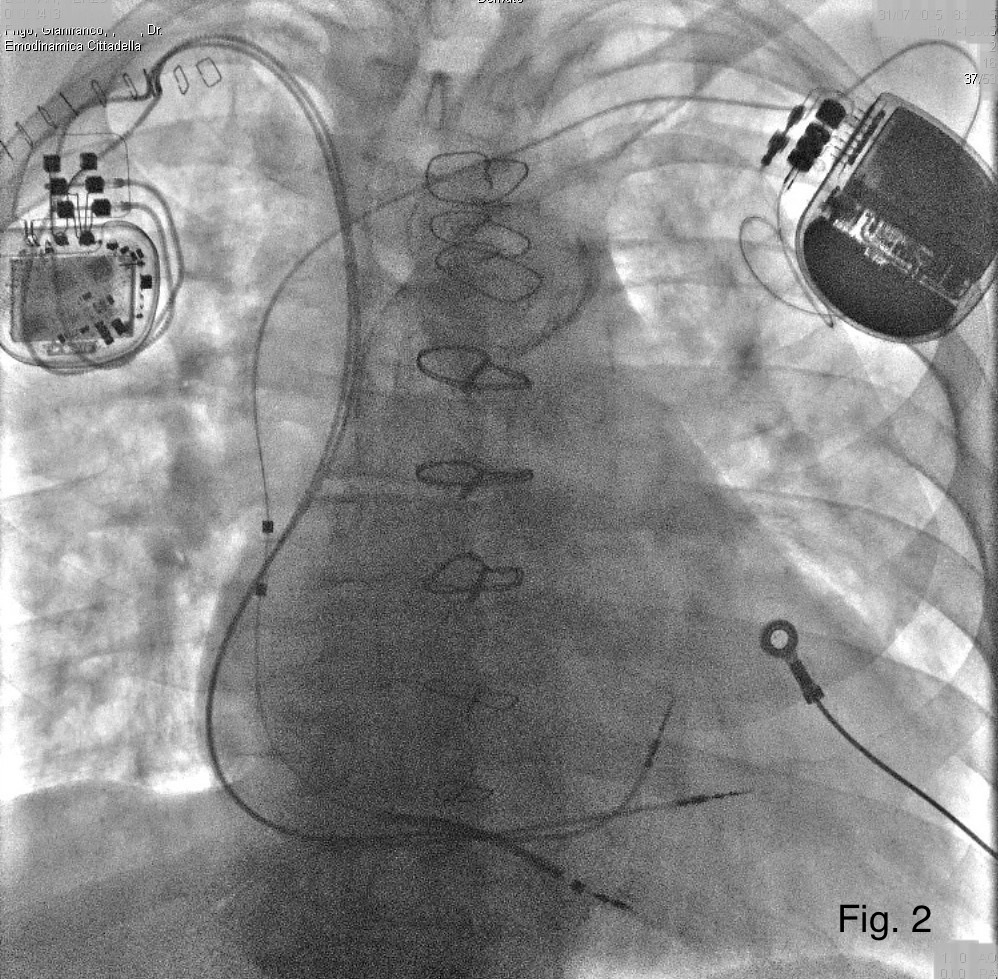
Background: Subclavian vein stenosis or occlusion represents a significant challenge during transvenous cardiac device implantation, potentially compromising lead placement and increasing procedural risk. In cardiac contractility modulation (CCM) therapy, it is common to implant the device with a concomitant contralateral pacemaker or defibrillator, thus involving both the right and left venous accesses. Case summary: We report the case of a 74-year-old gentleman, previously implanted for primary prevention with a single chamber ICD capable of atrial sensing (Biotronik, Acticor 7 VR-T DX). The patient with numerous cardiovascular risk factors, COPD and chronic renal failure, had ischemic heart disease with severely depressed ejection fraction and had previously undergone revascularization with coronary artery bypass grafting. The ICD was implanted on the left side. The patient was selected for a CCM device implant (Impulse Dynamics, Optimizer Smart Mini) due to worsening heart failure symptoms requiring recurrent hospitalizations. The right venography, performed before the procedure, revealed a stenotic/nearly occluded right subclavian vein (Fig. 1a-b). Using a fluoro-guided right axillary approach and gentle maneuvers, a guidewire was advanced into the partially patent vein and progressive venous dilation allowed safe advancement of the introducer sheath. Through the same access, the two active fixation leads were advanced toward the interventricular septum according to standard practice. Post-procedural imaging confirmed stable leads positioning and the absence of venous injury or thrombosis (Fig. 2) Discussion : This case highlights that, even in the presence of significant stenosis, with careful pre-procedural venous assessment and the use of gradual dilation techniques, transvenous pacing lead implantation may be feasible. The availability of guidewires of different softness and dilators of various calibers can be useful in a step-by-step approach to resolving the difficulty. In the case of CCM implantation concomitantly with another device, both venous accesses must be engaged, until an integrated technology is available. Conclusion : Partial stenosis/occlusion of the subclavian vein does not necessarily preclude successful pacemaker implantation, but the procedure may be challenging. The upcoming integrated CCM/HV technology will make it easier to manage cases with difficult anatomical variants such as the case described.