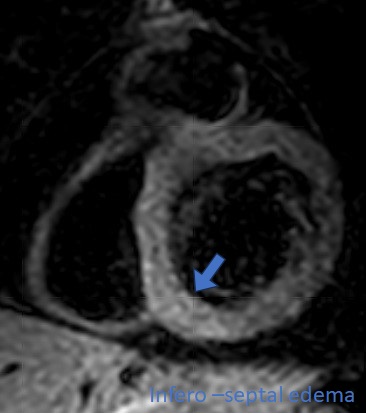
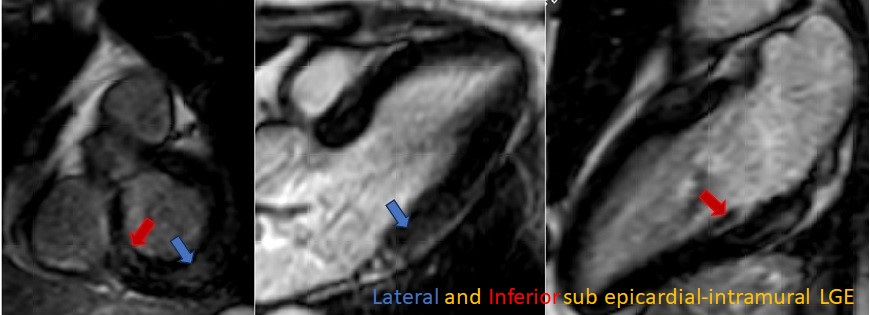
Introduction: Campylobacter Jejuni (C.J.) is a non-spore-forming, Gram-negative, microaerophilic, helical rod-shaped bacterial species commonly found in animal feces. It is commonly associated with poultry diseases and is one of the most common causes of gastroenteritis in humans worldwide. Improperly prepared beef and poultry are the most common ways of transmission. Very rarely, gastroenteritis is followed by chest pain indicative of myocarditis. Case report: A 33-year-old female patient with a latex allergy and seasonal allergens developed gastroenteritis with diarrhea and fever. Seven days after the onset of gastrointestinal symptoms, she also developed pain in her left arm, which worsened the following day with the onset of oppressive retrosternal chest pain. The pain was continuous and only minimally affected by breathing. In Emergency room: normal EKG, WBC 10100 10 9 /L (4-9); Hb 122 g/L (135-170); PLT 344000 10 9 /L (150-400), creatinine 0.59 mg/dl (0.59-1.04), K 3.3 mmol/L (3.6-5.2), Na 138 mmol/L (135-145), TnI 2445 ng/L (< 50) CRP 30 mg/L (< 3.3). EchocardioCD: normal. Cardiac MRI: Active non-ischemic inflammatory damage at the lower basal site, with partial involvement of the lower septum and posterior and lateral wall. Positive stool culture for C.J. Anti-inflammatory therapy with aspirin 500 mg three times a day with improvement of chest pain and azithromycin for 3 days was started. No arrhythmias were observed on telemetry throughout the entire hospital stay. EKG on discharge: "Flat" T wave in V5-V6. Conclusions: C.J. myocarditis is a very rare complication of the more common C.J. gastroenteritis. The evolution, as in this case, is usually benign. In rare cases, however, it can progress to more complex forms, and one related death has been reported in literature. The onset of cardiac symptoms during gastroenteritis should always lead to a diagnosis of IMPS (inflammatory myopericardial syndrome). EKG, echocardiogram, and troponin measurement are first-level tests. If troponin is abnormal, even in the absence of EKG or echocardiogram changes, the investigations should be complemented with cardiac MRI, which often reveals an inflammatory pattern not visible with other methods. A stool culture is also useful as it can reveal the causative agent, allowing for the setting of targeted antibiotic therapy