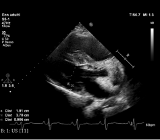
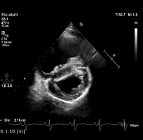
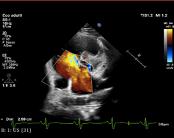
We present a case of a 41-year-old patient with Down syndrome who was admitted to ED due to worsening dyspnea. Chest X-ray showed pulmonary congestion and an enlarged heart, while echocardiography revealed left ventricular (LV) hypertrophy without outflow obstruction, severe dilation of the right ventricle (RV), and an interatrial septal defect. Following stabilization, the patient was referred for further evaluation, presenting with moderate dyspnea and no ongoing home therapy. The EKG showed sinus rhythm, left anterior hemiblock, RBBB, signs of left heart overload, negative T waves in V4-V6. Echocardiography confirmed a large ostium primum atrial septal defect with a left-to-right shunt, a hypertrophic LV, a cleft left atrioventricular valve with mild insufficiency. The RV was dilated but normocontractile, with moderate insufficiency of the right atrioventricular valve. Pulmonary artery systolic pressure was estimated at 52 mmHg, with dilation of the pulmonary trunk and branches and D-shape. These findings were consistent with a transitional-type atrioventricular canal defect, significant atrial septal defect, right heart overload, and pulmonary hypertension, along with non-obstructive HCM. Cardiac MRI revealed extensive patchy endomyocardial LGE in hypertrophic LV segments, papillary muscles, and both ventricular junctions, along with subendocardial LGE on the right side of the middle basal septum and trabeculae of the right ventricle. Right heart catheterization was performed to assess hemodynamic status, diagnosing pulmonary hypertension with both precapillary and postcapillary components, which was reversible. A low-dose outpatient diuretic therapy was initiated, and regular follow-up was established, leading to improvements in symptoms and exercise capacity. Congenital heart defects are common in individuals with Down syndrome, but hypertrophic cardiomyopathy is rare, and its association with atrioventricular canal defects is even more uncommon. In cases like ours, where symptoms manifest in adulthood, the risk-benefit ratio of any corrective intervention must be carefully considered, particularly given the patient's reduced life expectancy compared to the general population. Initially, pharmacological management should be prioritized to control symptoms and regular follow-up visits should be conducted.