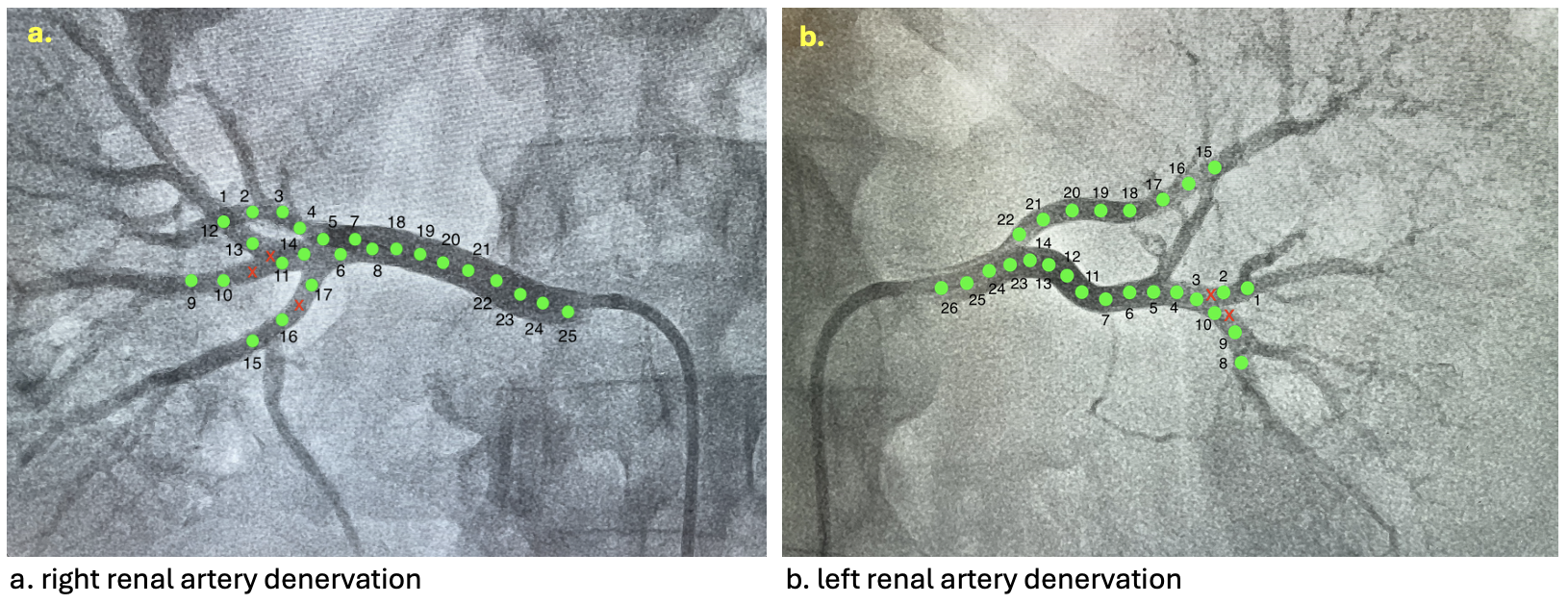
BACKGROUND Resistant arterial hypertension carries a high cardiovascular risk and remains challenging to control. Renal sympathetic denervation (RDN) is an interventional option for carefully selected patients. CLINICAL CASE A 58-year-old man presented with long-standing resistant arterial hypertension. Past medical history included recent NSTEMI treated with drug-coated balloon angioplasty, peripheral artery disease with moderate stenosis at the femoral-iliac bifurcation, dyslipidaemia, obesity, OSAS. At admission, blood pressure remained severely elevated with a non-dipping profile on 24h monitoring. Echocardiography showed preserved systolic function, severe left atrial enlargement, moderate diastolic dysfunction. A comprehensive diagnostic workup excluded secondary hypertension. According to the patient’s profile and a multidisciplinary evaluation (Cardiologist, Nephrologist, Anaesthesiologist), bilateral RDN was proposed. RDN was successfully performed using the Symplicity Spyral system (25 ablations on the right and 26 on the left – fig.1a and b), without complications. The in-hospital course was uneventful, with stable renal function and no arrhythmias. Our patient was safely discharged with a follow-up appointment in 3 months with 24h blood pressure monitoring showing good pressure control without hypertensive peaks. CONCLUSIONS This case highlights the role of RDN as an effective and safe adjunctive therapy in carefully selected patients. In a complex clinical setting characterized by multiple comorbidities, RDN was successfully performed without procedural complications, short-term adverse events or negative impact on renal function. This experience supports the feasibility of RDN in high-risk patients, reinforcing its value as a therapeutic option when conventional strategies fail. DISCUSSION Resistant arterial hypertension remains a clinical challenge, as it is associated with an increased risk of cardiovascular morbidity and mortality. Despite advances in pharmacological therapy, a subset of patients continues to exhibit inadequate blood pressure control, often due to heightened sympathetic nervous system activity. RDN has re-emerged as a promising interventional strategy. Secondary causes of hypertension must be excluded, fulfilling one of the key prerequisites for considering RDN. The decision-making process always involves a multidisciplinary team, underscoring the importance of appropriate patient selection and shared clinical judgment.