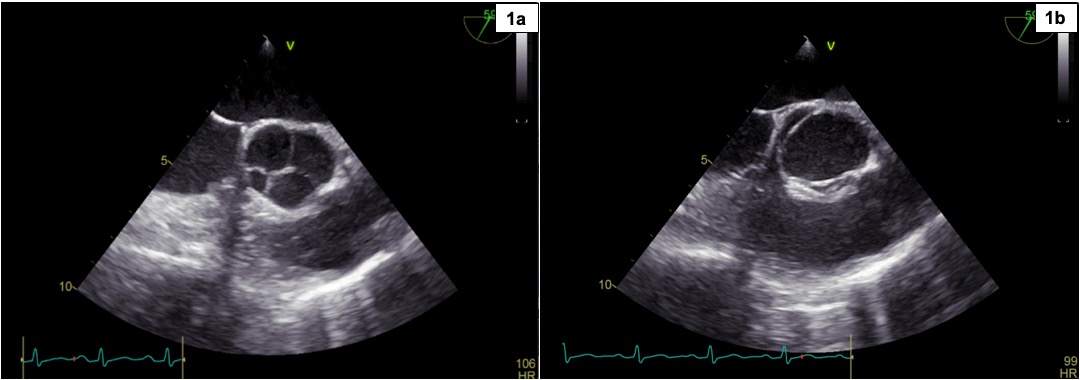
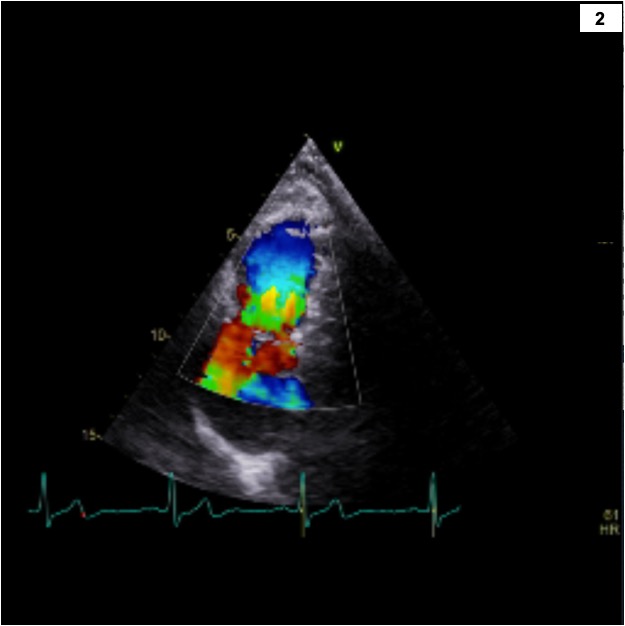
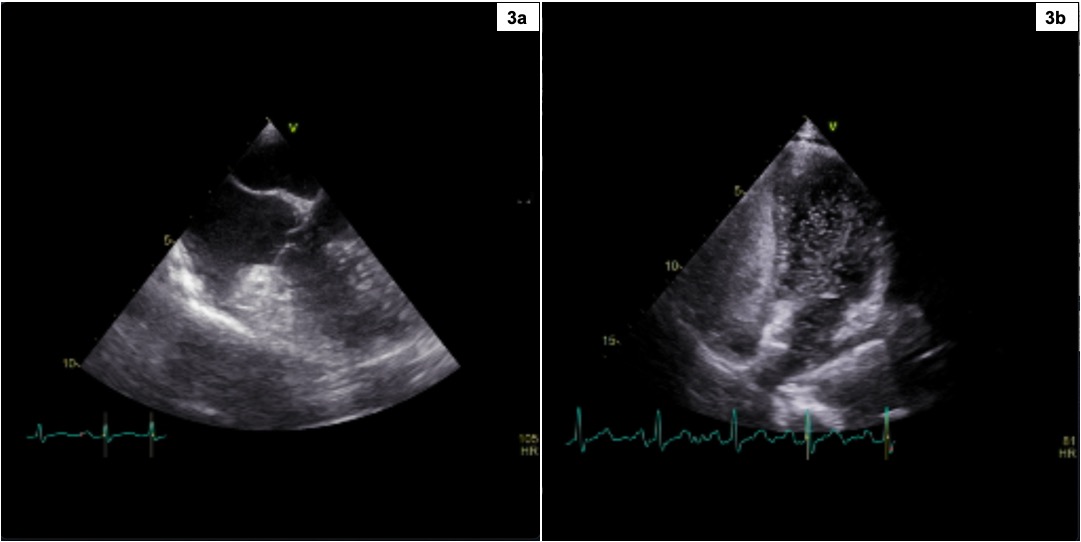
INTRODUCTION: Quadricuspid aortic valve (QAV) is a rare congenital anomaly characterized by the presence of four cusps of varying possible dimensions. In symptomatic cases, it typically presents with progressive valve insufficiency, sometimes requiring valve replacement. QAV can be associated with additional congenital heart defects, generally represented by coronary anomalies. CLINICAL CASE: A 28-year-old woman presented to the cardiology clinic following a left cerebellar ischemic stroke that occurred without apparent cardiovascular risk factors or plausible causes. Transthoracic echocardiography integrated with transesophageal echocardiography revealed: a type B QAV according to Hurwitz and Roberts classification and type II according to Nakamura classification (1a), with preserved opening motion (1b) and no significant valve regurgitation. The aortic variant was associated with a thickened pulmonary valve with mild stenosis (2), characterized by a maximum transvalvular gradient of 22 mmHg related to the co-existence of a supravalvular membrane, and mild-to-moderate insufficiency. Additional findings included an ectasia of the distal trunk and proximal branches of the pulmonary arteries, as well as an aneurysm of the interatrial septum (3a), right-convex (1R), associated with a prominent Eustachian valve and Chiari network, with evidence of a patent foramen ovale (PFO) showing a large right-to-left shunt during bubble test with Valsalva maneuver (3b). Other echocardiographic findings were normal. Given the absence of other plausible etiological hypotheses for the ischemic stroke and a RoPE score of 10, the high-risk PFO was deemed the most probable cause. Consequently, the patient underwent closure of the PFO using an Amplatzer device. An echocardiographic follow-up program was also initiated to monitor potential progression of the aortic and pulmonary valve diseases and the pulmonary trunk ectasia. DISCUSSION: QAV is a rare congenital anatomical variant that, in approximately 18% of cases, can coexist with other congenital heart anomalies. The peculiarity of this clinical case lies in its association with pulmonary valve disease causing mild stenosis, ectasia of the pulmonary trunk, and an interatrial septal aneurysm with a high-risk PFO, likely the cause of the ischemic stroke. CONCLUSION: Echocardiographic imaging allowed for an accurate diagnosis of QAV associated with other congenital anomalies and guided an appropriate therapeutic approach.