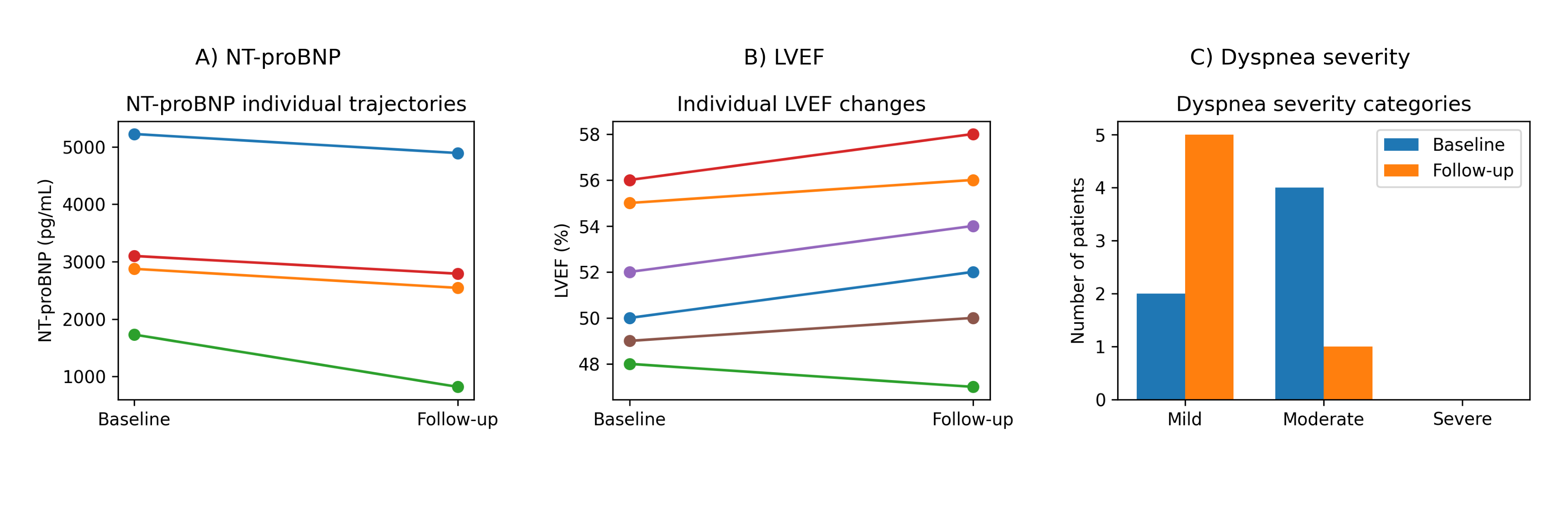
Background Transthyretin cardiac amyloidosis (ATTR-CM) is an increasingly recognised cause of heart failure in older adults, but real-world data in patients aged ≥80 years are limited. Methods A retrospective analysis was conducted on a real-world cohort of patients aged ≥80 years with cardiac amyloidosis, as part of routine clinical practice in Amyloidosis referral center in S. Camillo-Forlanini Hospital in Rome. A comprehensive data set was collected at the time of the initial evaluation and at the subsequent follow-up, as defined by the first available clinical reassessment following the initial evaluation during routine clinical practice. This included clinical characteristics, echocardiographic findings, biomarkers, electrocardiographic features and medical therapy. The functional status and cognitive performance of the subjects were systematically assessed. Results The population included 12 male patients with a median age of 82 years (IQR 80–85); follow-up data were available for 7 patients. At baseline, all patients were independent in activities of daily living and had preserved cognitive function. Symptoms of decompensation were frequent, with moderate to severe dyspnoea in approximately 75% of cases and peripheral oedema in over 80%. Left ventricular ejection fraction was generally preserved (median 52.5%), with increased wall thickness and typical echocardiographic findings of amyloidosis, including apical sparing. NTproBNP levels were markedly elevated. All patients with available data were treated with tafamidis, combined with diuretics and, in most cases, SGLT2 inhibitors. During the 6- and 12-month follow-up, despite incomplete data, there was no evidence of accelerated disease progression. NT-proBNP levels were stable or reduced in most patients, left ventricular systolic function remained stable, and a descriptive improvement in congestive symptoms was observed. There were no deaths or hospitalisations for heart failure. Conclusions In this real-world cohort of older adults aged ≥80 years with cardiac amyloidosis who were functionally and cognitively preserved, a contemporary therapeutic strategy was associated with clinical and biomarker stability over time. Despite the limits imposed by the sample size and incomplete follow-up data, our findings support the hypothesis that advanced age per se should not be considered a contraindication for active treatment.