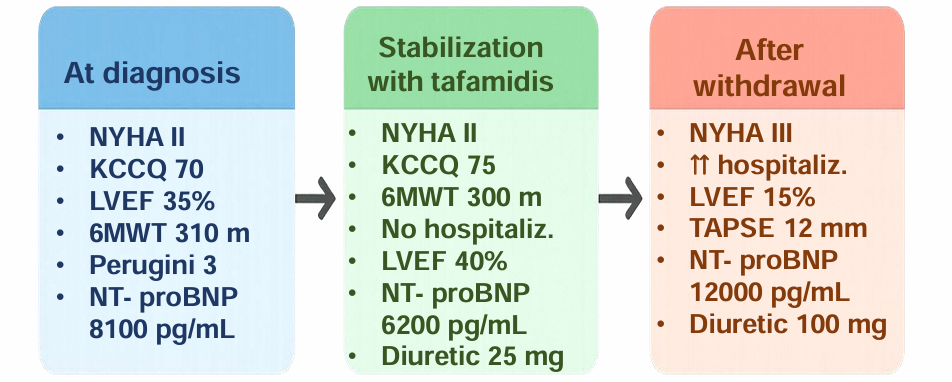
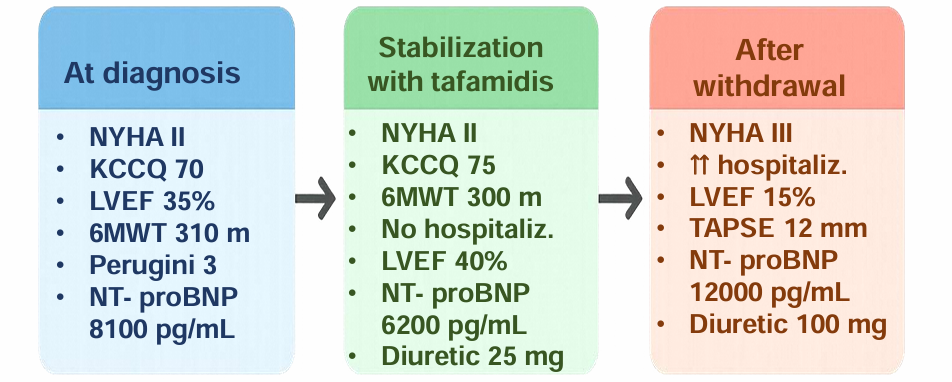
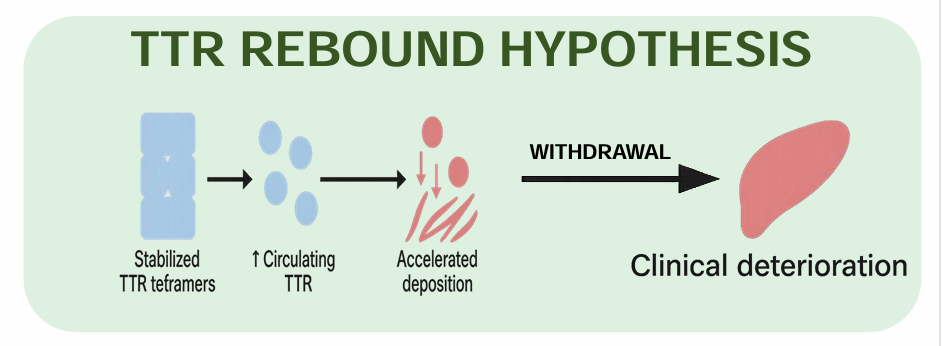
INTRODUCTION Wild-type transthyretin cardiac amyloidosis poses a therapeutic challenge, particularly in elderly patients, requiring a balance between clinical stability, treatment cost, and management complexity. CASE In 2016, an 82-year-old male patient was admitted to the Cardiology ward after experiencing precordial pain. Coronary angiography was negative for significant coronary stenoses. Echocardiography revealed mild left ventricular hypertrophy (12 mm), reduced left ventricular ejection fraction (LVEF 30%), grade I diastolic dysfunction. NT-proBNP was 599 pg/ and troponin negative. In 2019, echocardiography showed increased thickness of the interventricular septum (18 mm), LVEF 35%, and NT-proBNP levels of 6070 pg/mL. Bone scintigraphy demonstrated Perugini grade 3, TTR genetic test and hematologic screening were negative. In 2022, stability was observed. After AIFA approval, Tafamidis therapy was initiated. After 24-months, the patient showed clinical stability: interventricular septal thickness decreased (16 mm) and LVEF increased to 40%. The patient remained NYHA class II, completed a 6-minute walking test of 300 m, had a KCCQ score of 75, and NT-proBNP levels decreased to 6200 pg/mL. In July 2024, Tafamidis was discontinued due to advanced age and patient preference. Within a few months, the patient experienced rapid clinical deterioration, with frequent hospital admissions for heart failure, progression to NYHA class III symptoms, and increasing diuretic requirements (up to 100 mg of furosemide per day). Echocardiography revealed severe biventricular dysfunction (EF 15%, TAPSE 10 mm), elevated filling pressures (E/e′ 21). NT-proBNP and high-sensitivity troponin levels increased twofold (12,000 pg/mL and 84 ng/L). DISCUSSION Tafamidis has been shown to stabilize TTR tetramers, thereby preventing the formationof amyloid. However, it has also been demonstrated that this process concomitantly results in an increase in circulating TTR levels. Its abrupt discontinuation has been hypothesised to lead to rapid TTR deposition in myocardial tissue, potentially triggering acute decompensation. CONCLUSION This case demonstrates the capacity of Tafamidis to stabilise clinical status in ATTR-wt, but raises the alarm about a possible rebound effect after discontinuation. If confirmed, our hypothesis highlights the need for careful evaluation before initiating treatment in elderly and frail patients where any subsequent suspension could even be harmful.