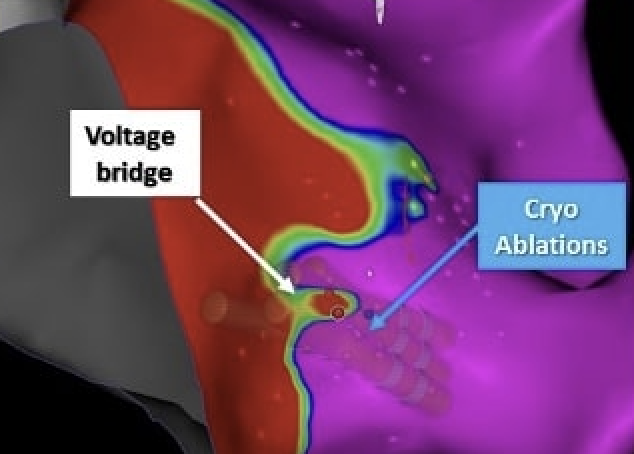
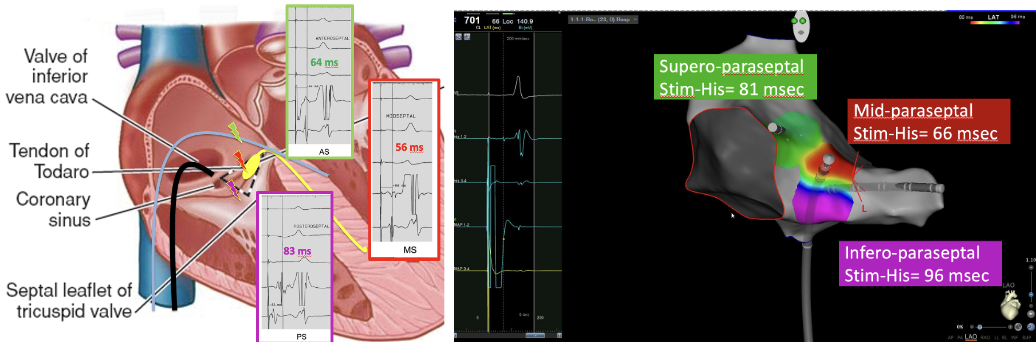
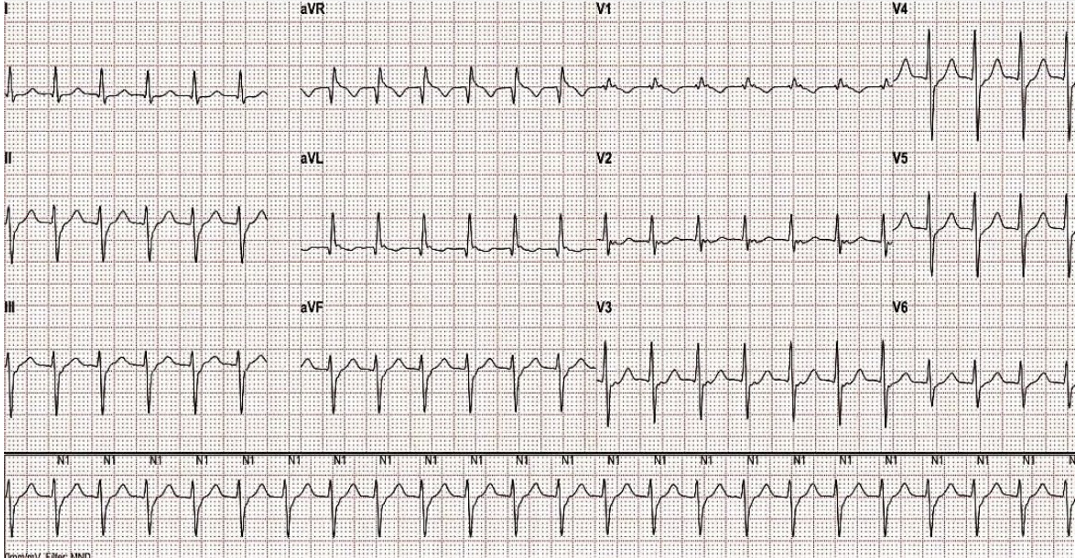
35-year-old male, active smoker, presented with recurrent episodes of palpitations. EKG showed sinus rhythm without pre-excitation or conduction disturbances. Ambulatory ECG recordings documented regular narrow QRS tachycardia with a short RP interval, consistent with supraventricular tachycardia. No structural heart disease and was referred for electrophysiological study and ablation. Noninvasive evaluation excluded ischemic and structural heart disease. Patient underwent an electrophysiological study using the PICENO AVNRT low-fluoroscopy protocol with the CARTO system. During the electrophysiological study, typical AV nodal re-entrant tachycardia (AVNRT) was induced and confirmed by ventricular pacing maneuvers. A 3D Koch’s Triangle Pace Mapping (KTPM) was performed to localize the compact AV node by measuring the stimulus-to-His (St–His) interval at different sites within Koch’s triangle. Unexpectedly, short St–His intervals were recorded in the mid-paraseptal region , while longer intervals were found in the antero-septal area indicating a mid-paraseptal extension of the compact AV node . Voltage Bridge Mapping (VBM) then identified a discrete low-voltage bridge connecting two high-voltage atrial areas in the same region, corresponding to the functional slow pathway . Because of the close proximity between the slow pathway and the compact node (identyfied via KTPM), cryoablation was selected to minimize the risk of iatrogenic atrioventricular block. Cryo-energy applications were delivered under 3D guidance at the VBM-defined low-voltage bridge site. Junctional beats appeared during freezing, indicating successful slow pathway modification. Post-ablation stimulation (baseline and isoproterenol challenge) showed no inducible AVNRT . The procedure was completed without fluoroscopy or complications , and the patient was discharged the day after. At 12-month follow-up, he remained asymptomatic and arrhythmia-free , with preserved AV conduction on ECG and Holter monitoring. This case illustrates the power of the PICENO AVNRT protocol , integrating KTPM and VBM to identify atypical compact AV nodal anatomy. Recognition of short St–His intervals in the mid-paraseptal zone revealed a mid-septal extension of the AV node , guiding the choice of cryoablation for safety. The fully 3D-guided, zero-fluoroscopy workflow allowed effective slow pathway modification while preventing AV block—underscoring its value in anatomically complex AVNRT cases.