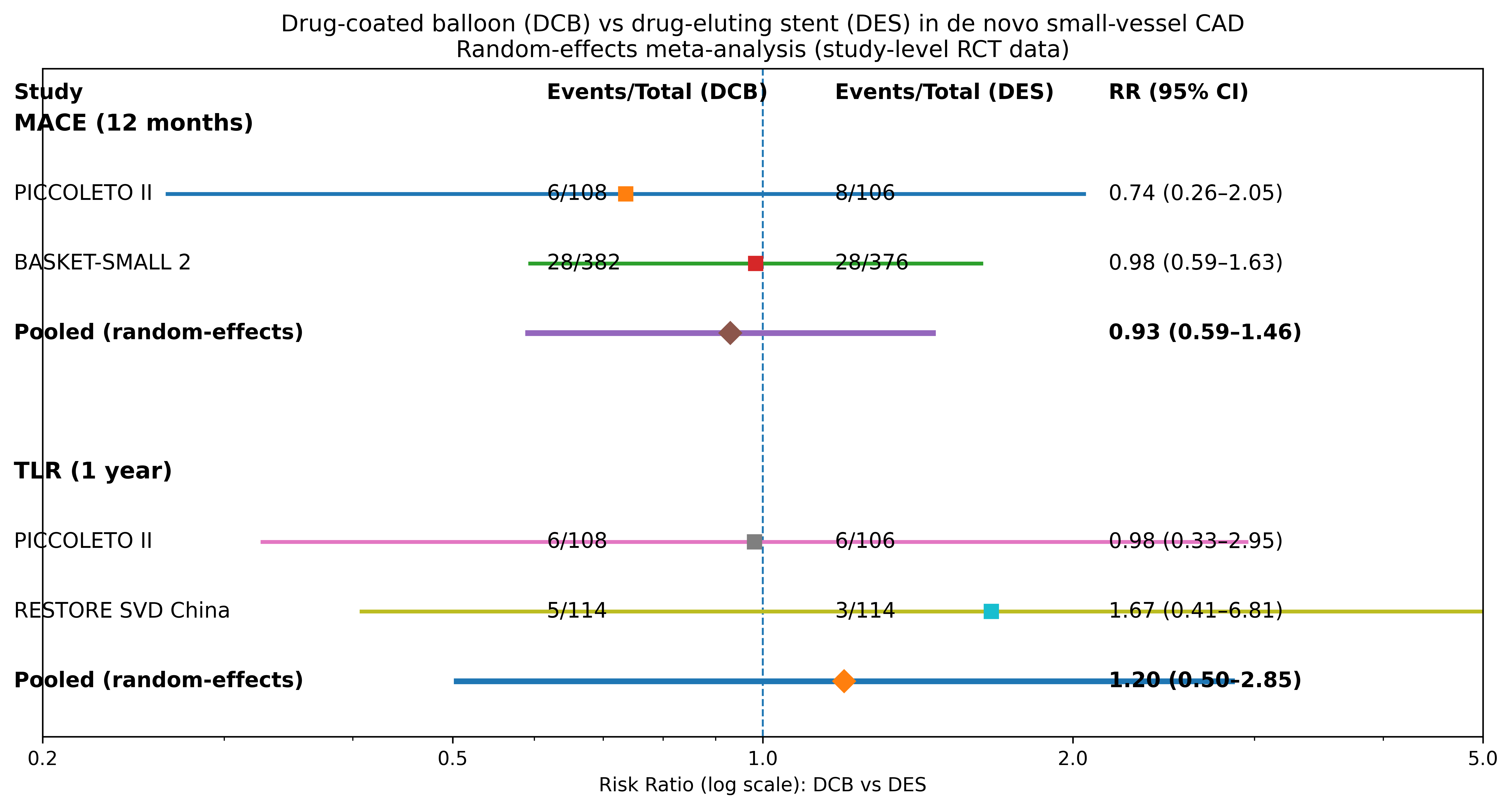
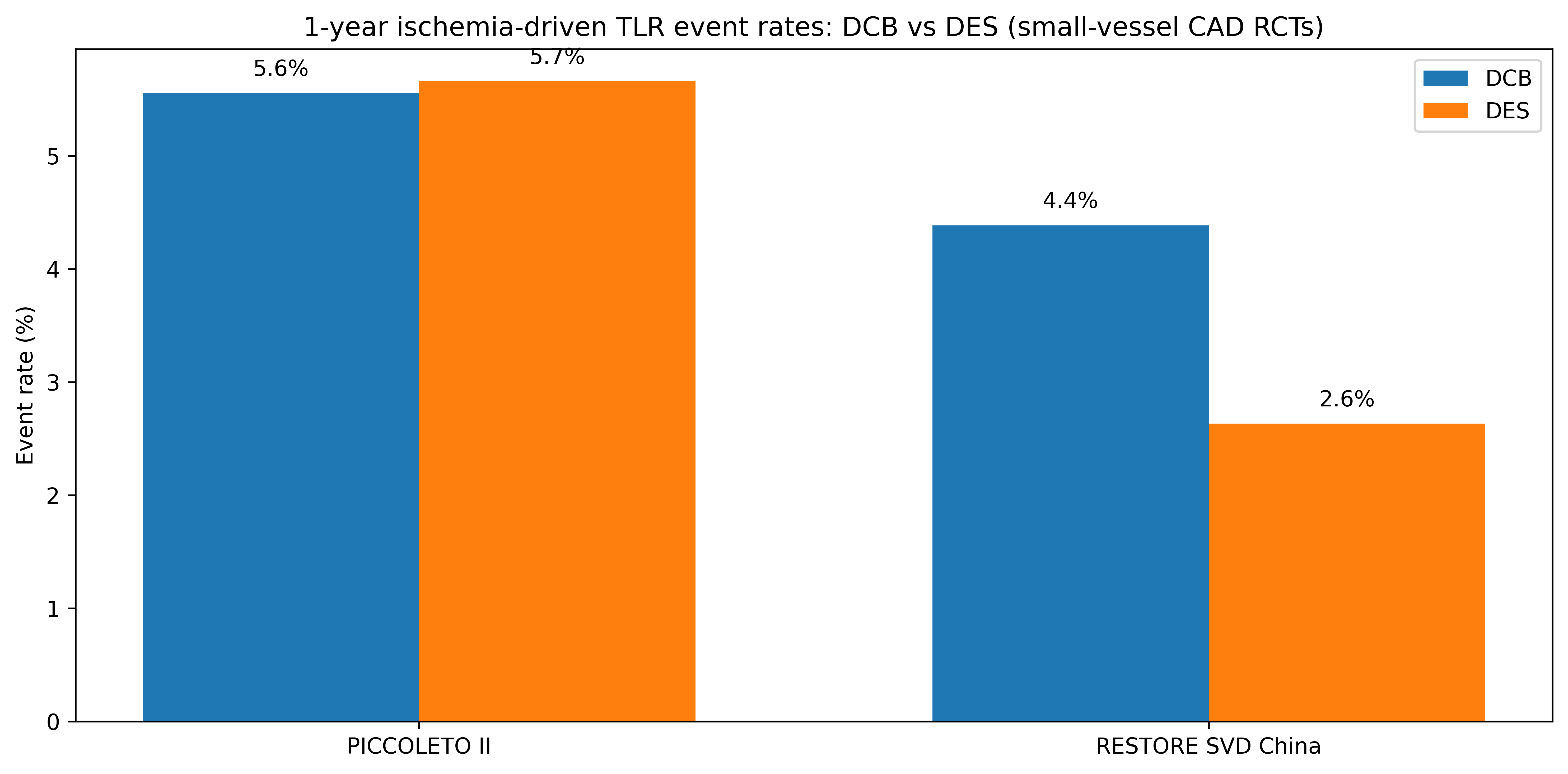
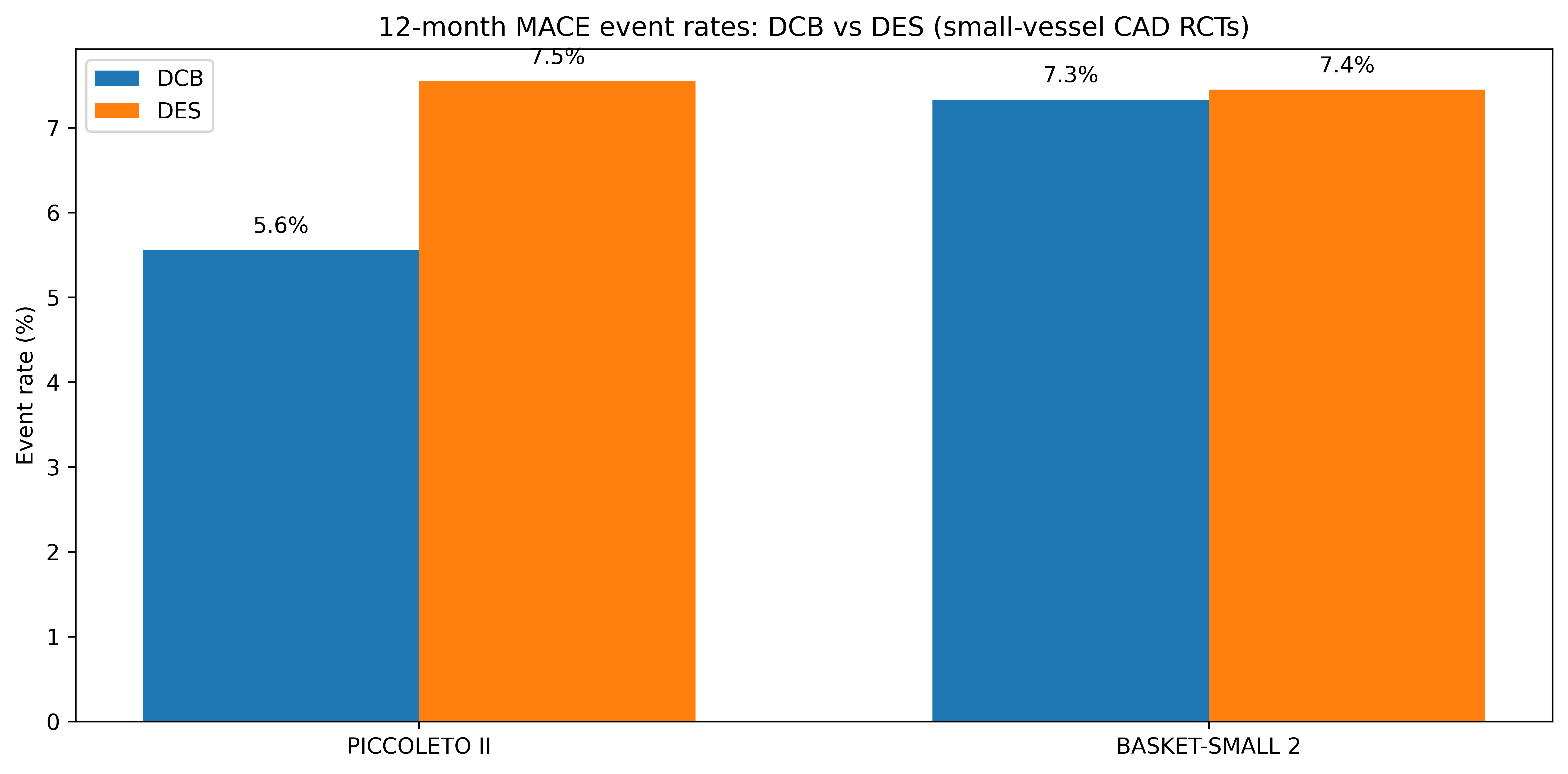
BACKGROUND Drug-coated balloons (DCB) enable a “leave-nothing-behind” strategy in de novo small-vessel coronary disease, potentially reducing metal burden while maintaining efficacy. We synthesized randomized evidence versus contemporary drug-eluting stents (DES). METHODS Systematic search for randomized controlled trials comparing DCB-only versus DES in de novo small coronary vessels (≤3.0 mm). Primary endpoint: 12-month major adverse cardiac events (MACE; trial-defined). Secondary endpoint: ischemia-driven target lesion revascularization (TLR) when available. Risk ratios (RR) were pooled using a random-effects model; heterogeneity was assessed with I². RESULTS Two trials reporting comparable 12-month MACE were included (n=972). In PICCOLETO II, MACE occurred in 6/108 (5.6%) with DCB and 8/106 (7.5%) with DES. In BASKET-SMALL 2, 12-month MACE was 7.5% with DCB and 7.3% with DES. Overall, DCB was not associated with a difference in MACE versus DES (pooled RR 0.99, 95% CI 0.63–1.55; I²=0%). For ischemia-driven TLR (2 trials, n=442), rates were low: PICCOLETO II 6/108 (5.6%) vs 6/106 (5.6%); RESTORE SVD China 5/114 (4.4%) vs 3/114 (2.6%). The pooled RR for ischemia-driven TLR was 1.20 (95% CI 0.50–2.85; I²=0%). CONCLUSIONS In de novo small-vessel PCI, DCB and contemporary DES showed comparable 12-month clinical outcomes with low revascularization rates. DCB appears a reasonable alternative in selected lesions, warranting larger trials powered for patient-centered endpoints and standardized definitions.