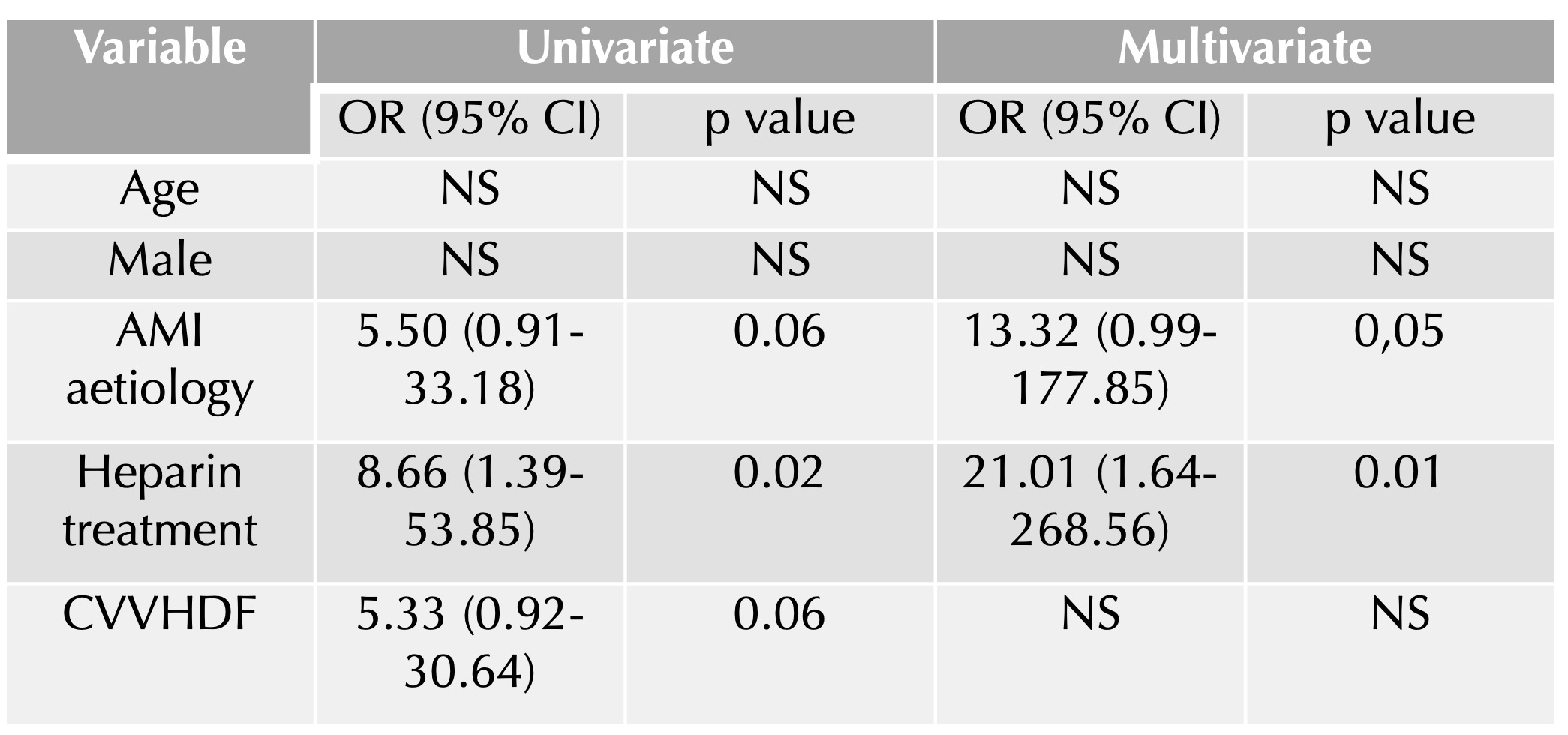
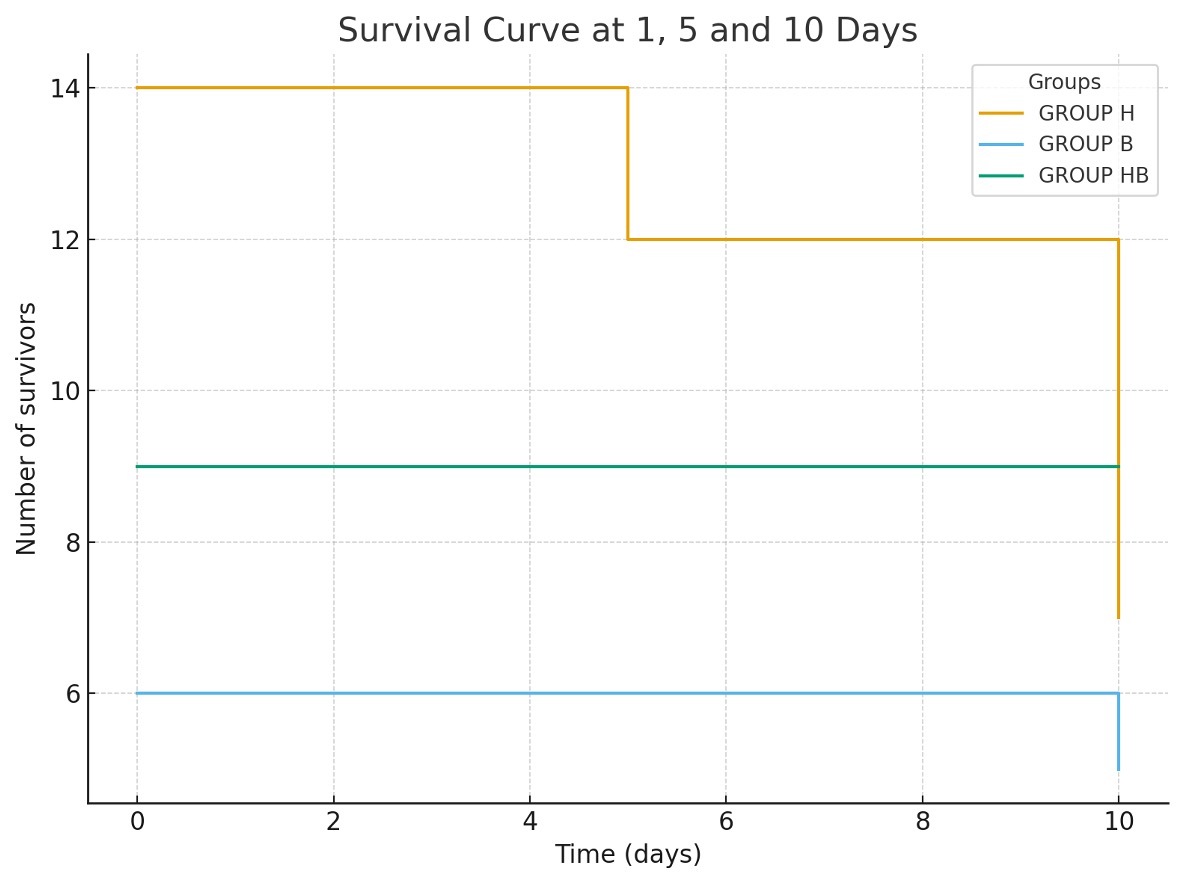
Background and aims : Cardiogenic shock is a severe, life-threatening condition often requiring VA-ECMO support. This study aimed to compare the safety and effectiveness of bivalirudin versus heparin anticoagulation in adults with cardiogenic shock on VA-ECMO. Methods : 29 consecutive patients were enrolled in this retrospective monocentre study between April 2021 and July 2025. All patients were treated with veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for cardiogenic shock and were admitted to our institution in Siena. Clinical features, short-term outcomes and laboratory data were collected. Results : Three sub-groups regarding anticoagulation strategies were identified: conventional heparin (H group, n=14), bivalirudin (B group, n=6), and an initial heparin regimen followed by a switch to bivalirudin (HB group, n=9). Baseline characteristics—including age (mean 57±10 years), aetiology (predominantly acute myocardial infarction, 55%), left ventricular ejection fraction (mean 14%), and SCAI stage (mostly D or E)—were comparable across groups. The HB group demonstrated the longest mean duration of ECLS support (13±8 days, p = 0.04 ). Use of central venting, adjunct mechanical unloading (IABP/Impella), and renal replacement therapy did not differ significantly between groups. Overall bleeding complications occurred in 31% of patients, thrombotic events were uncommon, and stroke occurred in 17% of the cohort, with similar distribution among groups. Transfusion requirements for blood products also showed no significant differences. Overall mortality was 48.2% and did not significantly differ across groups. However, mortality during ECMO support was significantly higher in the heparin group (57.1%, p = 0.01 ), whereas both bivalirudin-containing groups exhibited better early survival with no deaths recorded in the first 10 days. Survival analysis confirmed a significantly worse early trajectory for the heparin group ( p = 0.02, Figure 1) . Heparin treatment was significantly associated with higher in-hospital mortality on ECMO in univariable analysis (OR 8.66, p=0,02) and in multivariable analysis (OR 21.01, p=0,01), together with AMI aetiology (OR 13.32, p=0,05) ( Table 1 ). Conclusions : patients with cardiogenic shock on VA-ECMO treated with heparin experienced higher early mortality compared with those treated with bivalirudin or hybrid regimens. Heparin use and AMI aetiology were identified as independent predictors of death during ECMO support.