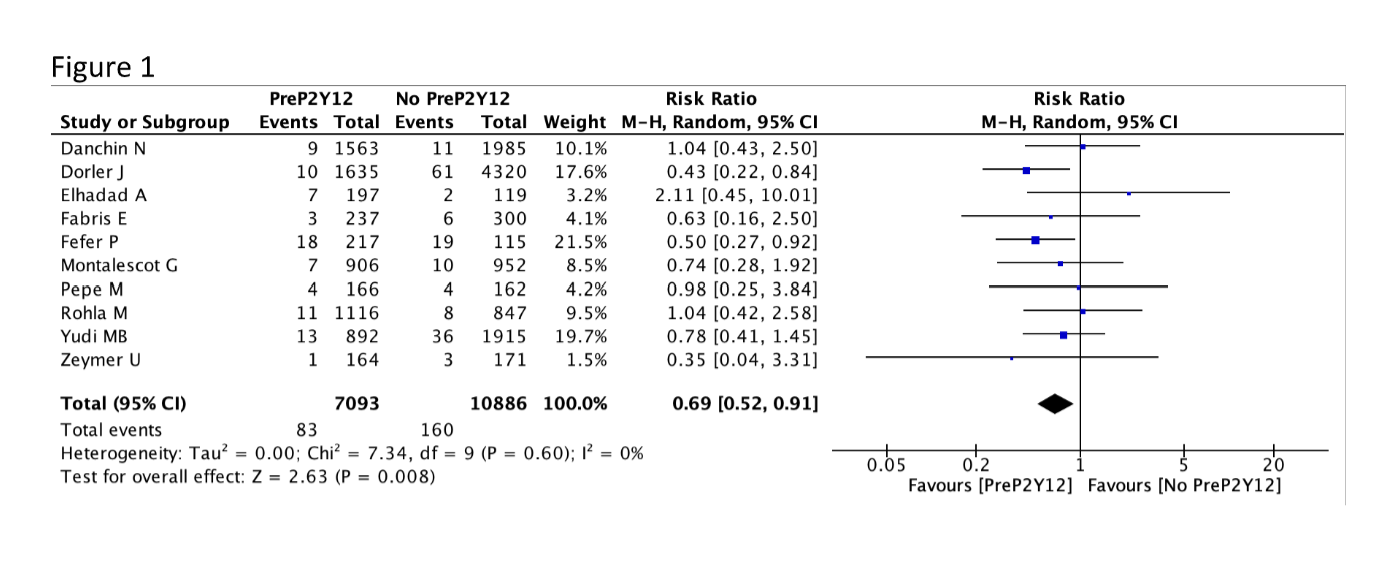
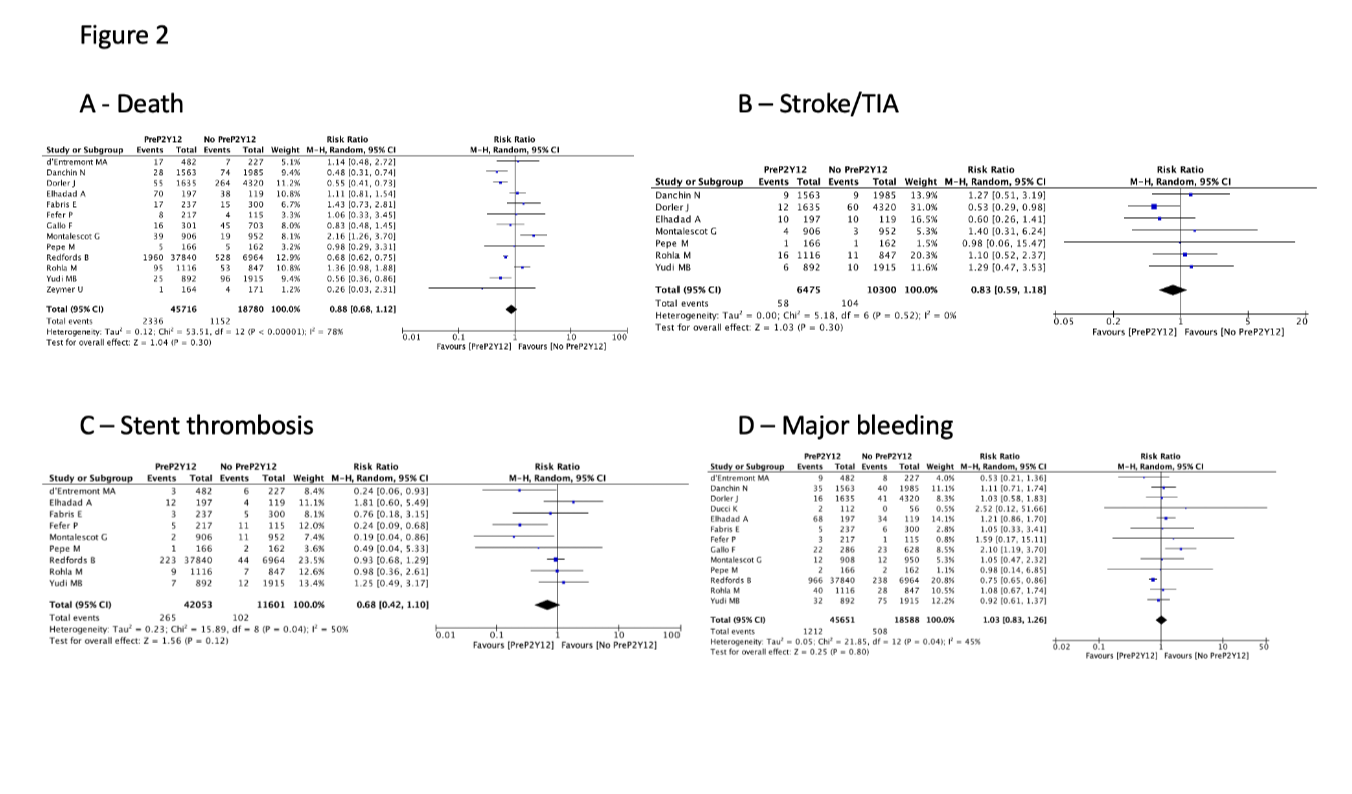
Introduction Although current European Society of Cardiology guidelines state that a P2Y12 inhibitor pretreatment strategy may be considered in STEMI patients undergoing a primary percutaneous coronary intervention (PCI) strategy (Class IIb), solid evidence to support this choice in clinical practice remains lacking. The aim of this study was to summarize the latest available evidence on this topic. Methods Electronic databases were searched for observational and randomized studies (RCT) comparing P2Y12 inhibitor pretreatment strategy versus downstream strategy (i.e., loading dose administered at the time of primary PCI) in patients with STEMI candidate to primary PCI. The studied outcomes were early reinfarction, death, stroke, stent thrombosis, and major bleeding. The statistical software Review Manager 5.4 was used to conduct a random-effect study-level metanalysis. The overall effect was reported as risk ratio (RR) and relative 95% confidence interval (CI). Results After the selection process a total of 15 studies (3 RCT, 1 post-hoc analysis of RCT and 11 observational) including 65.144 patients (45.915 pretreated and 19.227 no pretreated) were included in our analysis. The mean age of the included patients was 64±2 years and the mean reported time between P2Y12 administration and primary PCI in the pretreated group was 63±24 minutes. Patients pretreated with a P2Y12 inhibitor had a statistically significant lower risk of early reinfarction as compared with patients treated with P2Y12 at the time primary PCI (RR 0,69; 95% CI 0,52-0,91; p=0,008 – Figure 1). No significant differences were detected for the risk of death (RR 0,88; 95% CI 0,68-1,12; p=0,30), stroke (RR 0,83; 95% CI 0,59-1,18; p=0,30), stent thrombosis (RR 0,68; 95% CI 0,42-1,10; p=0,12), and major bleeding (RR 1,03; 95% CI 0,83-1,26; p=0,80) – Figure 2. Conclusion The results of our study-level meta-analysis suggest that a P2Y12 inhibitor pretreatment strategy in STEMI patients undergoing primary PCI may be associated with a reduced risk of early reinfarction, without a significant increase in the risk of major bleeding. Further studies are warranted to evaluate the impact of the time interval between P2Y12 inhibitor loading and primary PCI on clinical outcomes in pretreated patients.