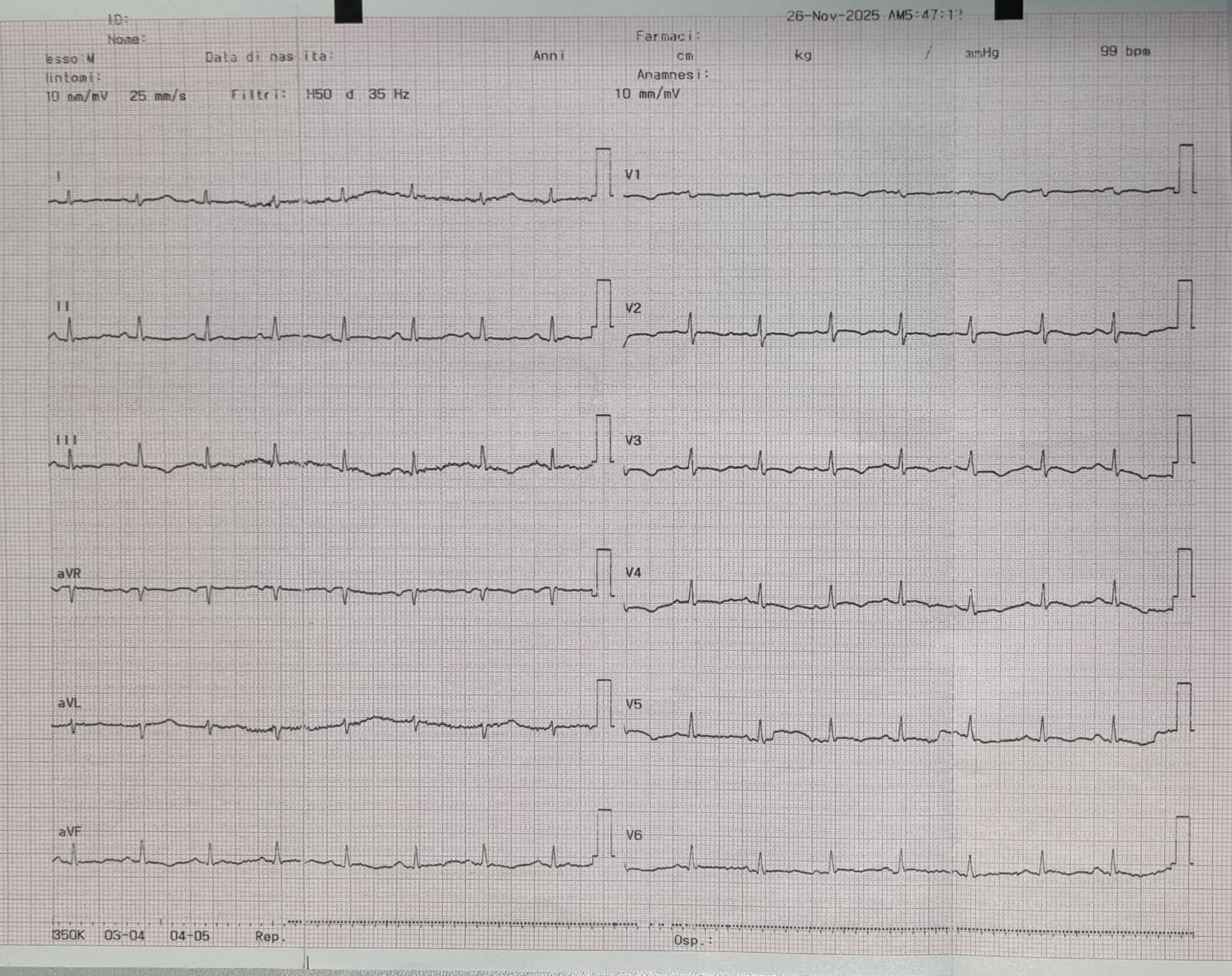
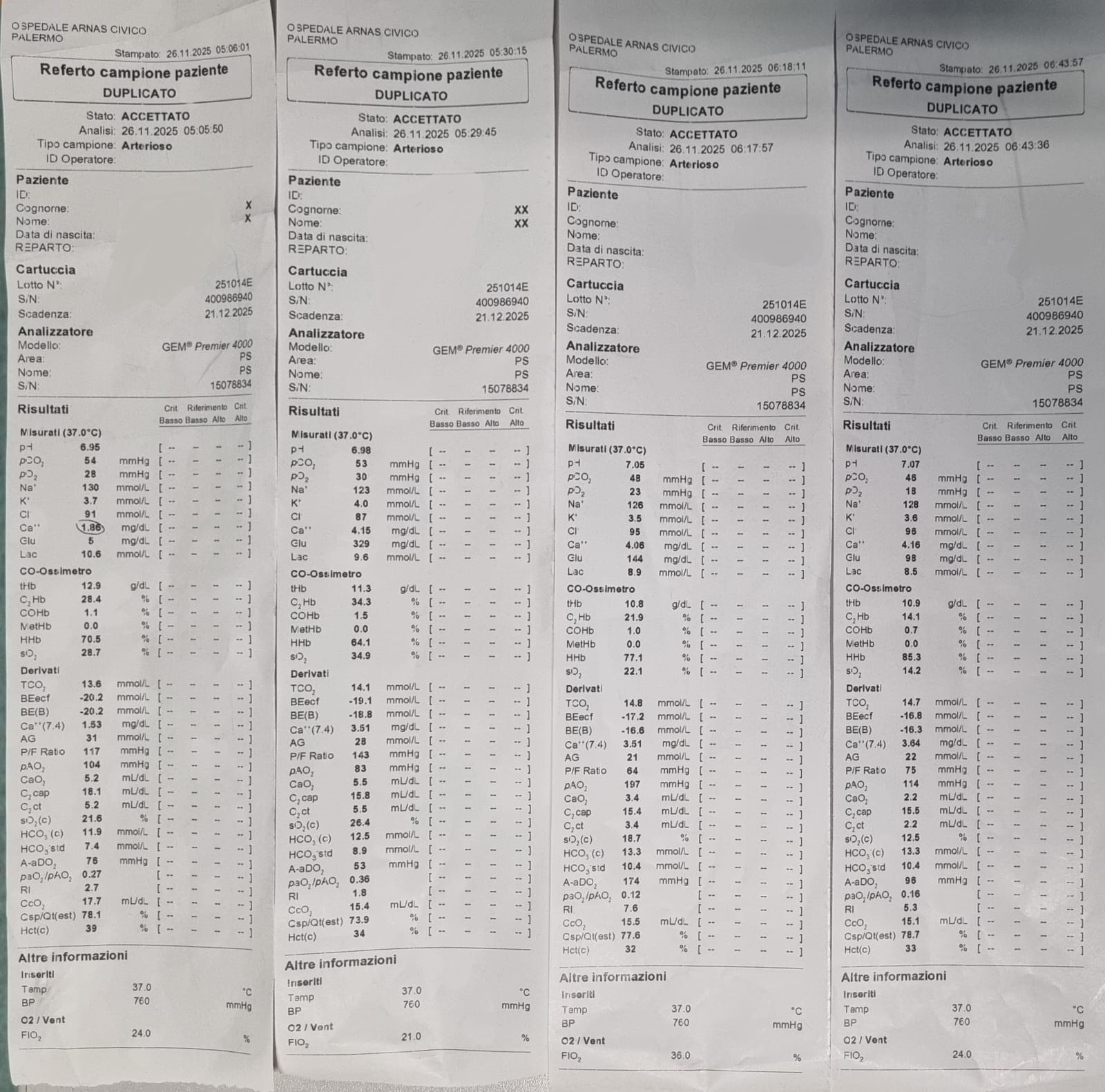
A 19-year-old woman was admitted to the Emergency Department for generalized tonic–clonic seizures after one week of fever. On admission she was comatose (GCS 3), hemodynamically stable, nonspecific abnormalities on ECG, and severe hypoglycaemia (5 mg/dL). Neurological status improved after intravenous glucose. Brain CT was unremarkable. Laboratory tests showed lymphocytic leukocytosis, elevated C-reactive protein, thrombocytopenia, mild troponin elevation, acute kidney injury, prolonged INR, mildly increased transaminases, and elevated LDH, CK and myoglobin. Two hours later, the patient developed sudden cardiac arrest due to pulseless electrical activity. Advanced life support and endotracheal intubation were initiated. Transthoracic echocardiography revealed a massive pericardial effusion causing cardiac tamponade. Emergency pericardiocentesis drained exudative fluid; however, refractory cardiac arrest persisted, with only a brief return of spontaneous circulation followed by prolonged electromechanical dissociation. After prolonged resuscitation, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was initiated. Early echocardiography showed severe biventricular dysfunction with minimal aortic valve opening, prompting IABP implantation for left ventricular venting. Given the suspicion of acute myopericarditis, high-dose corticosteroids were administered; endomyocardial biopsy was not feasible. Cardiac function rapidly improved, with normalization of biventricular systolic function within 48–72 hours, allowing ECMO weaning. Weaning was complicated by Harlequin syndrome, requiring urgent ECMO removal while maintaining IABP support, later discontinued. Extensive microbiological testing was negative.The ICU course was complicated by left lower limb compartment syndrome requiring fasciotomy, mild intracranial hemorrhagic suffusion during unfractionated heparin therapy, and pneumonia with pleural effusion. The patient recovered and was extubated without neurological sequelae. Cardiac magnetic resonance imaging performed after 15 days showed pericardial edema, circumferential effusion and diffuse late gadolinium enhancement of the pericardial layers, without myocardial involvement, consistent with acute pericarditis. The final diagnosis was acute myopericarditis complicated by cardiac tamponade, multiorgan dysfunction and severe transient post-arrest biventricular stunning, with a possible contribution of systemic inflammatory response syndrome.