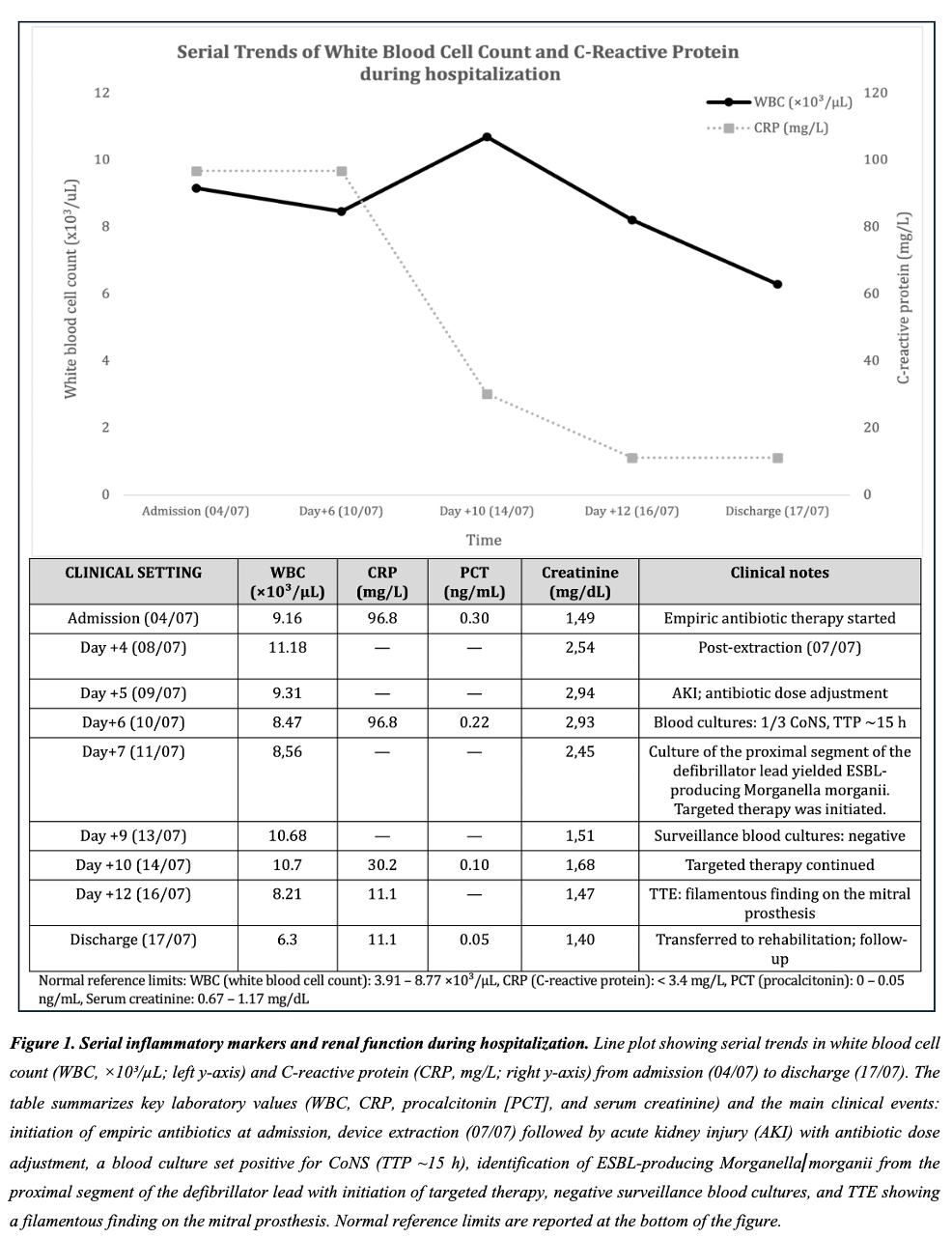
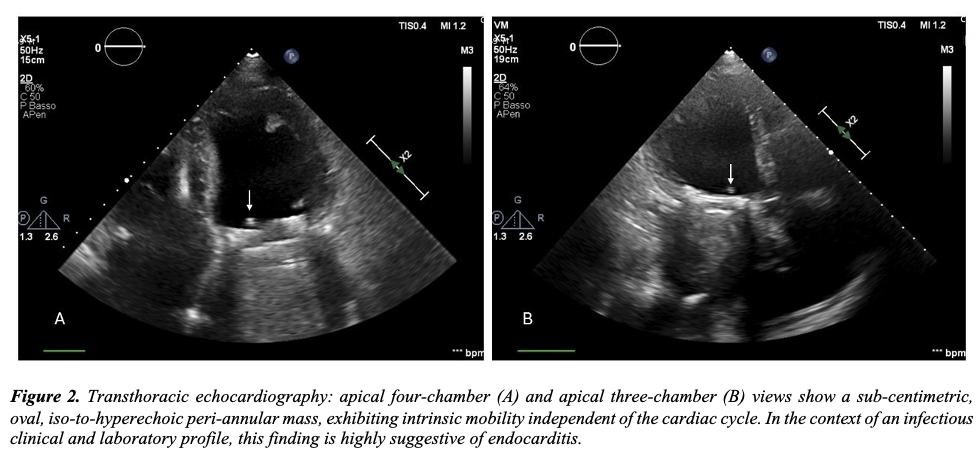
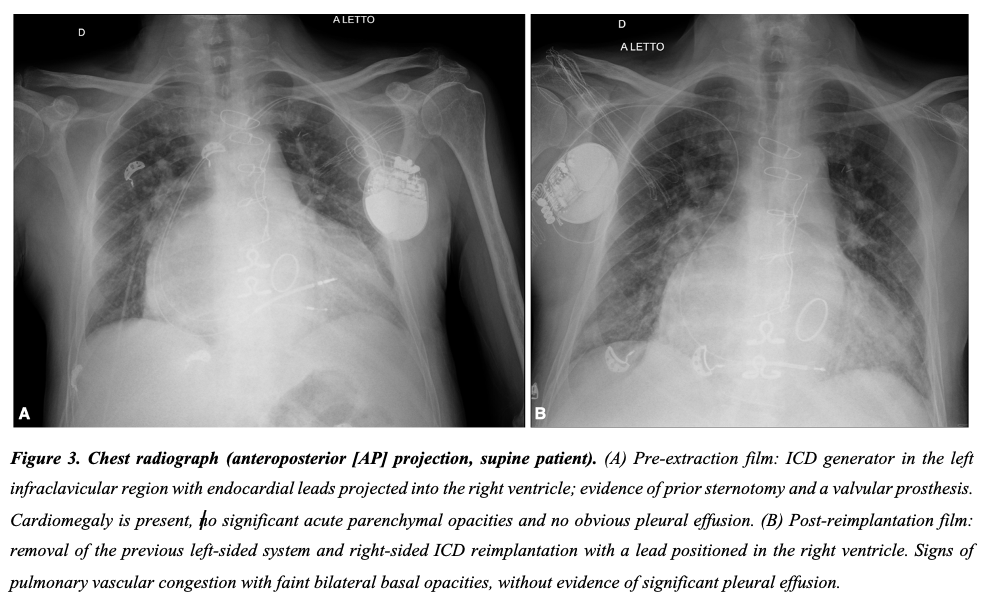
BACKGROUND: Cardiac implantable electronic device (CIED) infections are most often caused by staphylococci and, once established, usually require complete hardware removal. Gram-negative pathogens are uncommon; when ESBL producers are involved, timely targeted therapy and reimplant planning become even more challenging. CASE PRESENTATION: A 75-year-old man with diabetes, stage 3 chronic kidney disease, permanent atrial fibrillation on warfarin and a mechanical mitral prosthesis underwent ICD upgrade for worsening left ventricular function. After an early wound bleed treated in the community, he developed pocket dehiscence with generator exposure. He was clinically stable and afebrile, but inflammatory markers were markedly elevated. Empiric therapy with piperacillin/tazobactam plus daptomycin was started and blood cultures were obtained. Transthoracic echocardiography showed no definite endocarditis. The entire system was extracted, including an abandoned ventricular lead. A transient acute kidney injury required dose adjustment. One blood-culture set grew coagulase-negative staphylococci and was judged likely contamination after subsequent negative samples. Culture from the proximal defibrillator lead yielded ESBL-producing Morganella morganii, susceptible to carbapenems; therapy was switched to meropenem (renal-dosed) while continuing Gram-positive coverage. Given the arrhythmic risk and the absence of persistent bacteraemia, a contralateral single-chamber ICD was reimplanted a few days after extraction. Surveillance blood cultures remained negative. On follow-up echocardiography, a new small, mobile peri-annular mass adjacent to the mechanical mitral valve raised suspicion of prosthetic valve endocarditis, but the patient declined transoesophageal echocardiography and further imaging. He completed a prolonged antibiotic course, with falling inflammatory markers, renal recovery and good wound healing at 30–90 day follow-up. CONCLUSIONS: Even rare ESBL-producing Gram-negative organisms can underlie CIED infection. Complete extraction, rapid culture-driven escalation to a carbapenem, and careful dosing in renal dysfunction were key. In patients with prosthetic valves, a new post-extraction echocardiographic lesion should trigger an aggressive search for prosthetic valve endocarditis (TEE or alternative imaging when needed), even when cultures turn negative after antibiotics.