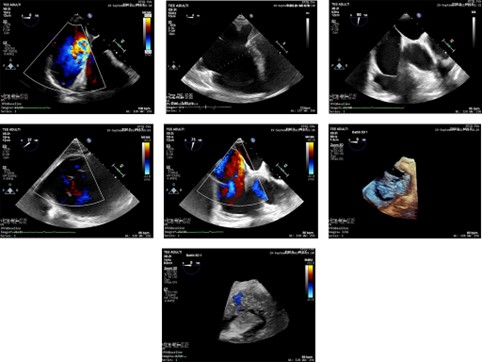
A 62-year-old male presented for a routine cardiovascular check-up, reporting palpitations and mild physical limitations (NYHA class II) but denying prior trauma or significant illnesses. Clinical examination revealed jugular venous distension and peripheral edema, suggesting underlying cardiac dysfunction. ECG showed sinus rhythm with P-wave anomalies. Transthoracic echocardiography (TTE) revealed marked dilation of the right atrium (61 ml/m²) and right ventricle, with severe eccentric tricuspid regurgitation (TR) directed towards the interatrial septum (IAS) and structural abnormalities of the tricuspid valve (TV) posterior leaflet. Doppler studies confirmed pathological TR (velocity > 2.8 m/s). Transesophageal echocardiography (TEE) identified severe TR (grade 4+/4) due to posterior leaflet prolapse, significant annular dilation (50 mm), and malcoaptation. Measurements, including a vena contracta >7 mm and convergence zone area of 13 mm, corroborated TR severity. The right ventricular function was preserved, and mild left ventricular diastolic dysfunction (E/E' <14) was noted. Differential diagnoses, including Ebstein’s anomaly, rheumatic disease, endocarditis, and implant-related issues, were excluded. Coronary angiography ruled out ischemic contributions. The patient underwent tricuspid valve repair via median sternotomy. Using an MC3 annuloplasty ring, the procedure corrected the posterior leaflet prolapse through annular plication, restoring leaflet coaptation. The choice of technique reflected the anatomical integrity of the anterior and septal leaflets, as "edge-to-edge" repair would have been required in their involvement due to significant annular dilation. At six months post-surgery, follow-up echocardiography confirmed complete resolution of TR, normalization of right atrial size, and no residual stenosis or regurgitation. The patient reported marked clinical improvement, with resolution of palpitations and peripheral edema. Although the etiology of TR initially remained unclear, subsequent discussions revealed that the patient had sustained unreported chest trauma during a car accident a year prior. The trauma likely exacerbated underlying myxomatous changes in the valve, resulting in posterior leaflet damage and severe TR.