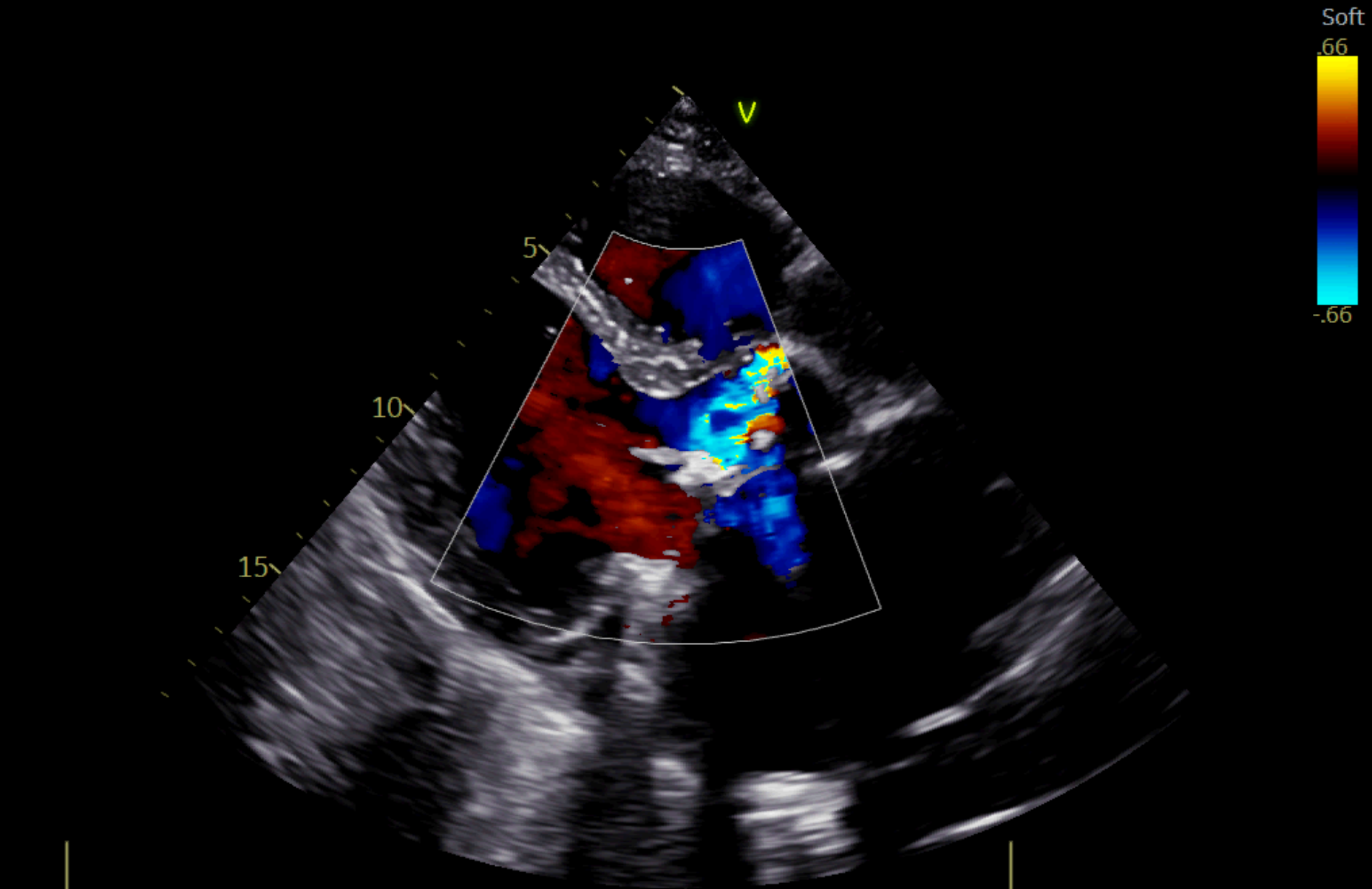
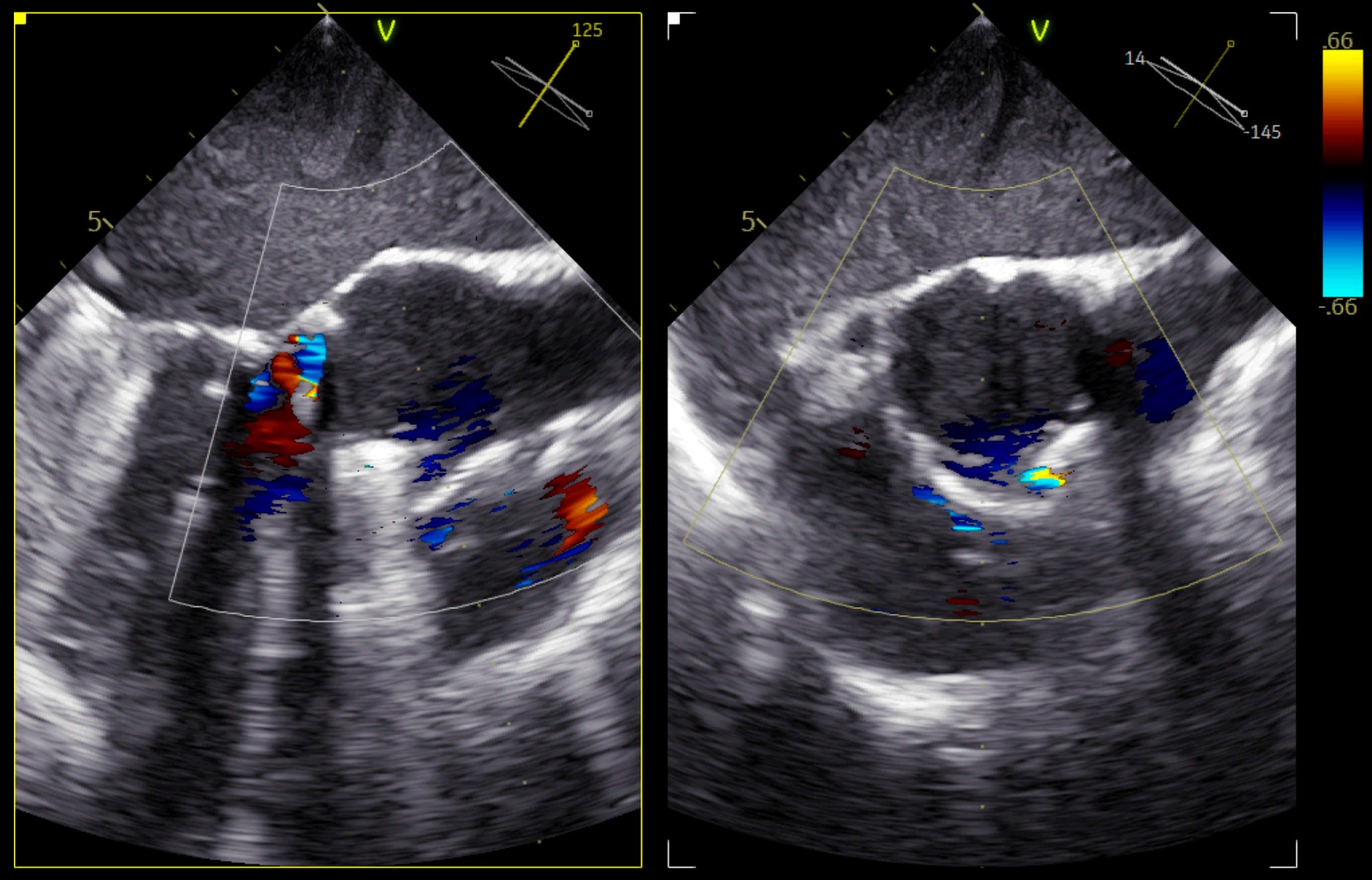
The Yacoub technique is a valve-sparing procedure for ascending aorta replacement, preserving part of the aortic root and remodeling it with a Dacron graft to maintain the anatomy of the Valsalva sinuses. We present the case of 64-year-old man with past medical history significant for Marfan syndrome with pectus excavatum, ascending aorta replacement due to aneurysm via Yacoub procedure (2000), subsequent aortic and mitral valve replacement with mechanical prostheses due to severe insufficiency (2006) and pacemaker implantation for total AV block (2019). He presented to the emergency department for chest pain, elevated cardiac troponin (5925 ng/L) and an INR of 2.1. Initial ECG revealed ventricular activity induced by a pacemaker. Transthoracic echocardiography showed apical and distal interventicular septum hypokinesia and a pseudoaneurysm of the aortic root near the right coronary sinus, communicating with left ventricular outflow tract and inducing significant volume overload. Left ventricular systolic function was borderline preserved (EF 50%) with mild chamber dilation. Chest CT confirmed a periprosthetic leak (14 × 9 mm) and showed a thrombus in the left atrial appendage. Coronary angiography demonstrated angiographically normal coronary arteries and aortography revealed severe paravalvular aortic regurgitation. Transesophageal echocardiography showed a crescent-shaped periannular image involving the right and non-coronary sinuses, consistent with severe paravalvular regurgitation. The clinical presentation, in the absence of significant coronary artery disease, was attributed to possible thromboembolic coronary event with spontaneous resolution. The periprosthetic leak, likely due to partial detachment of the mechanical valve on the remodeled aortic root, was deemed unsuitable for surgical correction due to the high risk of mortality of a third reoperation and associated severe pectus excavatum. Given the patient’s asymptomatic status, a strategy of close clinical and instrumental follow-up was adopted. This case highlights two potential complications faced by patients who underwent the Yacoub procedure followed by subsequent mechanical valve replacement. These include the high thromboembolic risk associated with prosthetic valves and inadequate anticoagulation and valve failure (in this case a perivalvular complication), as the aortic root remains at partially native and thus prone to the tissue laxity characteristic of Marfan syndrome.