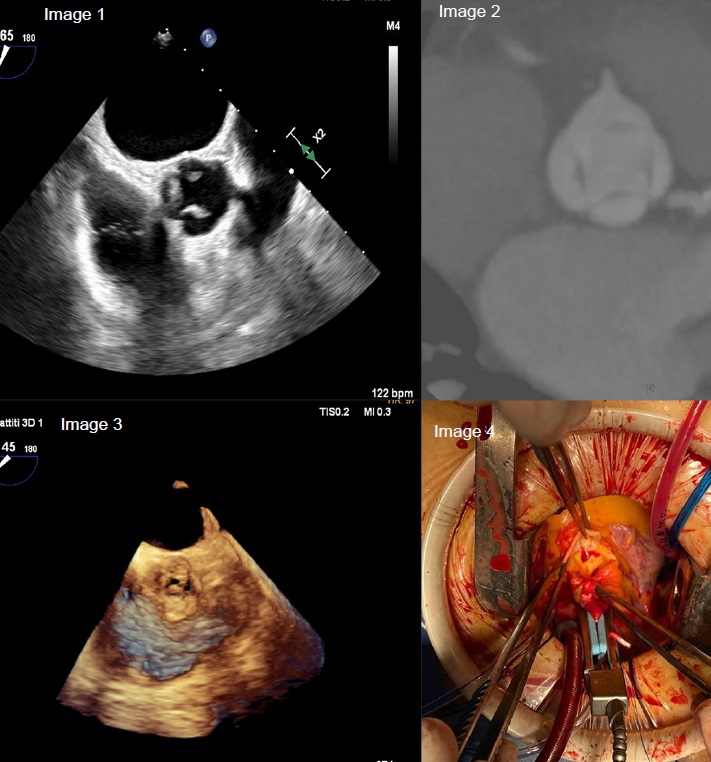
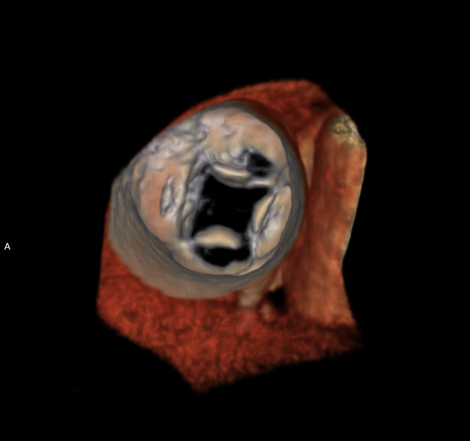
A 54-year-old woman presented in February 2024 with exertional dyspnea. She had no significant medical history, was a non-smoker, and denied medication use. Electrocardiography revealed left ventricular hypertrophy, while transthoracic echocardiography (TTE) showed an enlarged left ventricular cavity (end-diastolic diameter 54 mm) with normal wall thickness and preserved systolic function (ejection fraction 65%). The diastolic function was impaired with a relaxation pattern, but filling pressures were normal. The TTE also revealed severe aortic insufficiency due to central regurgitation, but the aortic root (33 mm) and ascending aorta (34 mm) were normal, and there were no other valvular abnormalities. Preoperative transesophageal echocardiography (TEE) confirmed a quadricuspid aortic valve (QAV) with four equal cusps, classified as type A according to Hurwitz and Roberts. Both 2D and 3D imaging, as well as computed tomography (CT), corroborated the findings and excluded coronary artery disease. Given the valve's complex morphology, the patient's relatively young age, and the low surgical risk, the heart team recommended surgical valve replacement over transcatheter aortic valve implantation. A 21 mm Inspiris Resilia bioprosthesis was implanted via mini-sternotomy. Intraoperative findings confirmed the quadricuspid valve, which had two right, one left, and one non-coronary cusp. The procedure lasted 3 hours and 40 minutes, and the patient was hospitalized for 14 days, including 2 days in the cardiology ICU. There were no complications, and the post-operative transesophageal examination confirmed the proper function of the prosthetic valve with a mean transvalvular gradient of 13 mmHg and no paravalvular leaks. At the 3-month follow-up, the patient reported full resolution of symptoms. TTE showed normal cardiac dimensions and function, and the bioprosthetic valve continued to function without issues, maintaining the same gradient.