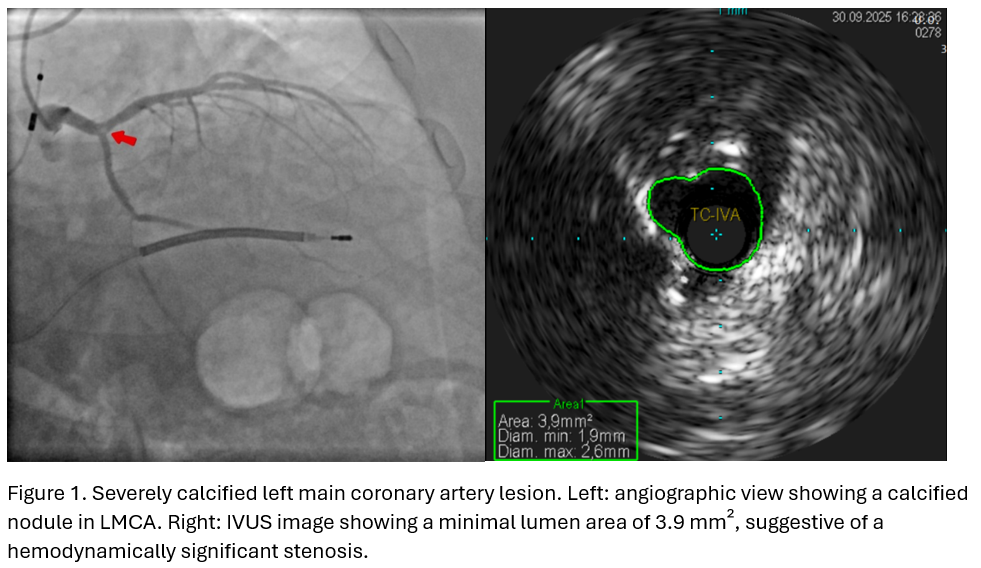
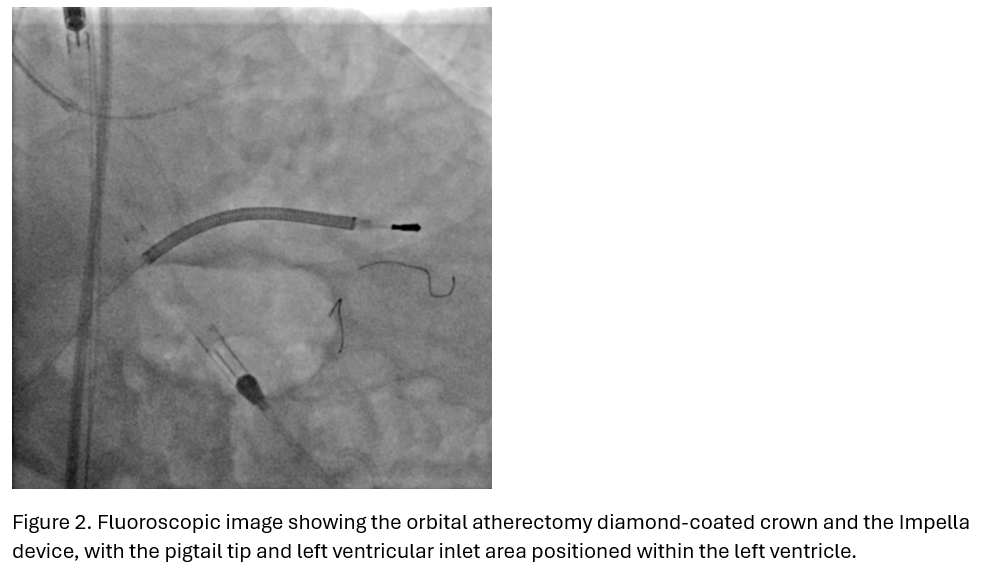
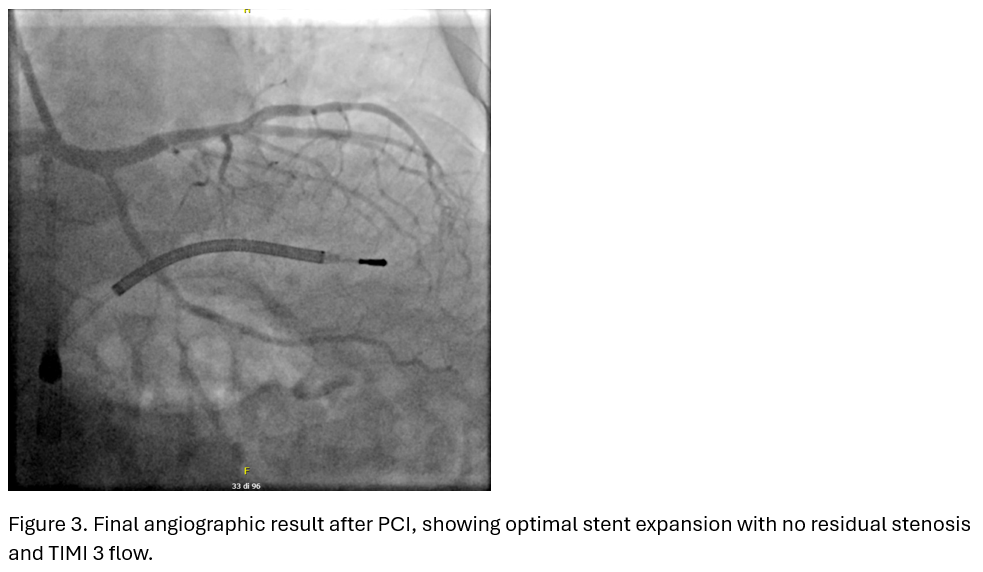
Background Calcified coronary lesions (CCL) represent a major challenge during percutaneous coronary intervention (PCI), particularly when involving the left main coronary artery (LMCA). Severe coronary calcification is associated with suboptimal stent expansion, malapposition, increased rates of restenosis, and a higher incidence of procedural complications. In this setting, the use of intravascular imaging and dedicated plaque-modifying strategies is often required to adequately prepare the lesion and optimize stent deployment. In patients with depressed left ventricular ejection fraction (LVEF) and complex coronary anatomy, high-risk PCI (HR-PCI), supported by percutaneous mechanical circulatory support (pMCS), may represent a viable alternative to coronary artery bypass grafting (CABG), particularly when surgical risk is deemed prohibitive. Case Summary We report the case of a 69-year-old man with multiple cardiovascular risk factors and chronic coronary syndrome, who was also an implantable cardioverter-defibrillator (ICD) carrier due to a prior history of ventricular arrhythmias. The patient presented with severe, heavily calcified, unprotected left main coronary artery (LMCA)–left anterior descending artery (LAD) bifurcation disease (Medina 1.1.0), in the setting of multivessel coronary artery disease and moderately reduced left ventricular ejection fraction (LVEF 40%). After Heart Team evaluation, CABG was ruled out because of excessively high surgical risk, and the patient was therefore referred for PCI. He underwent Impella-protected, intravascular ultrasound (IVUS)-guided PCI with orbital atherectomy and drug-eluting stent (DES) implantation from the LMCA into the LAD, followed by DES implantation in the mid-LAD. Post-procedural IVUS confirmed optimal stent expansion and apposition. No major periprocedural complications occurred. A planned angiographic follow-up performed two months later confirmed sustained patency of the LMCA–LAD and mid-LAD stents. Conclusions Orbital atherectomy allowed effective calcium modification, while IVUS guidance ensured adequate lesion assessment and stent optimization. Prophylactic Impella support mitigated hemodynamic risk in a patient with impaired ventricular function undergoing PCI of heavily calcified unprotected LMCA bifurcation disease. This case highlights the importance of careful patient selection, meticulous procedural planning and multimodality approach when considering high-risk PCI.