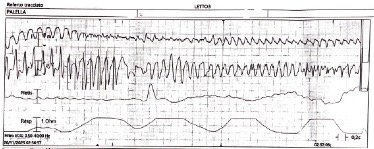
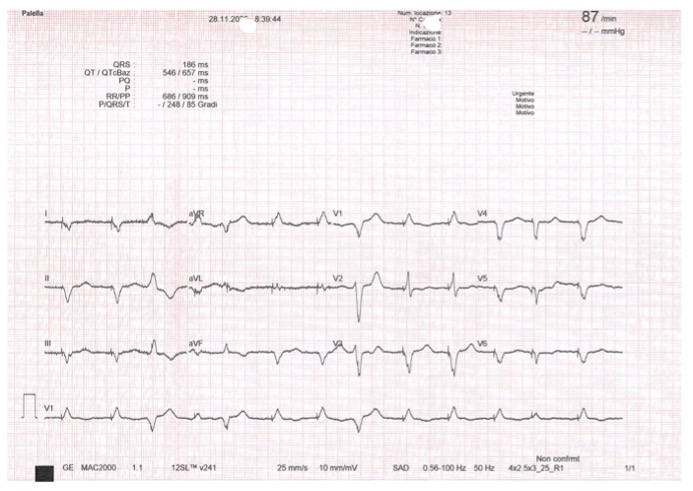
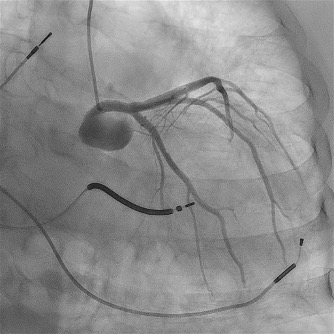
Background: Electrical storm (ES) and cardiogenic shock (CS) frequently coexist, sustaining a vicious cycle driven by sympathetic overactivation, malignant ventricular arrhythmias and hemodynamic collapse. Management is particularly challenging when beta-blockade and catecholamine escalation are limited by severe hypotension and pro-arrhythmic risk. Case report: A 74-year-old man with end-stage non-ischemic dilated cardiomyopathy, CRT-D, permanent atrial fibrillation and chronic kidney disease was admitted for ES with recurrent ventricular tachycardia and ventricular fibrillation requiring multiple appropriate ICD shocks. Despite treatment with metoprolol, magnesium, lidocaine and intravenous amiodarone, ES recurred and evolved into CS with mean arterial pressure of 50 mmHg, oliguria, acute kidney injury and rising lactate. Mechanical circulatory support was excluded because of advanced frailty. Given the high arrhythmic burden, escalation of norepinephrine was limited. Metoprolol was discontinued and intravenous landiolol, an ultra-short-acting and highly selective β 1-blocker, was cautiously introduced in association with continuous amiodarone infusion. To maintain adequate perfusion pressure without further adrenergic stimulation, arginine vasopressin was added to middle-dose norepinephrine. This combined strategy led to a reduction of sustained ventricular arrhythmias, restoration of electrical stability, improvement of mean arterial pressure above 65 mmHg, recovery of urine output and partial renal function improvement, allowing clinical stabilization and transfer to the regional arrhythmology center for ablation evaluation. Conclusions: This case supports the effectiveness and safety of intravenous landiolol, even in the setting of CS, for the control of refractory ES when combined with amiodarone. The adjunctive use of arginine vasopressin allowed hemodynamic stabilization while avoiding excessive norepinephrine dose escalation and its pro-arrhythmic effects. An integrated antiarrhythmic and hemodynamic approach may represent a valuable therapeutic option in selected high-risk patients with ES with concomitant CS.