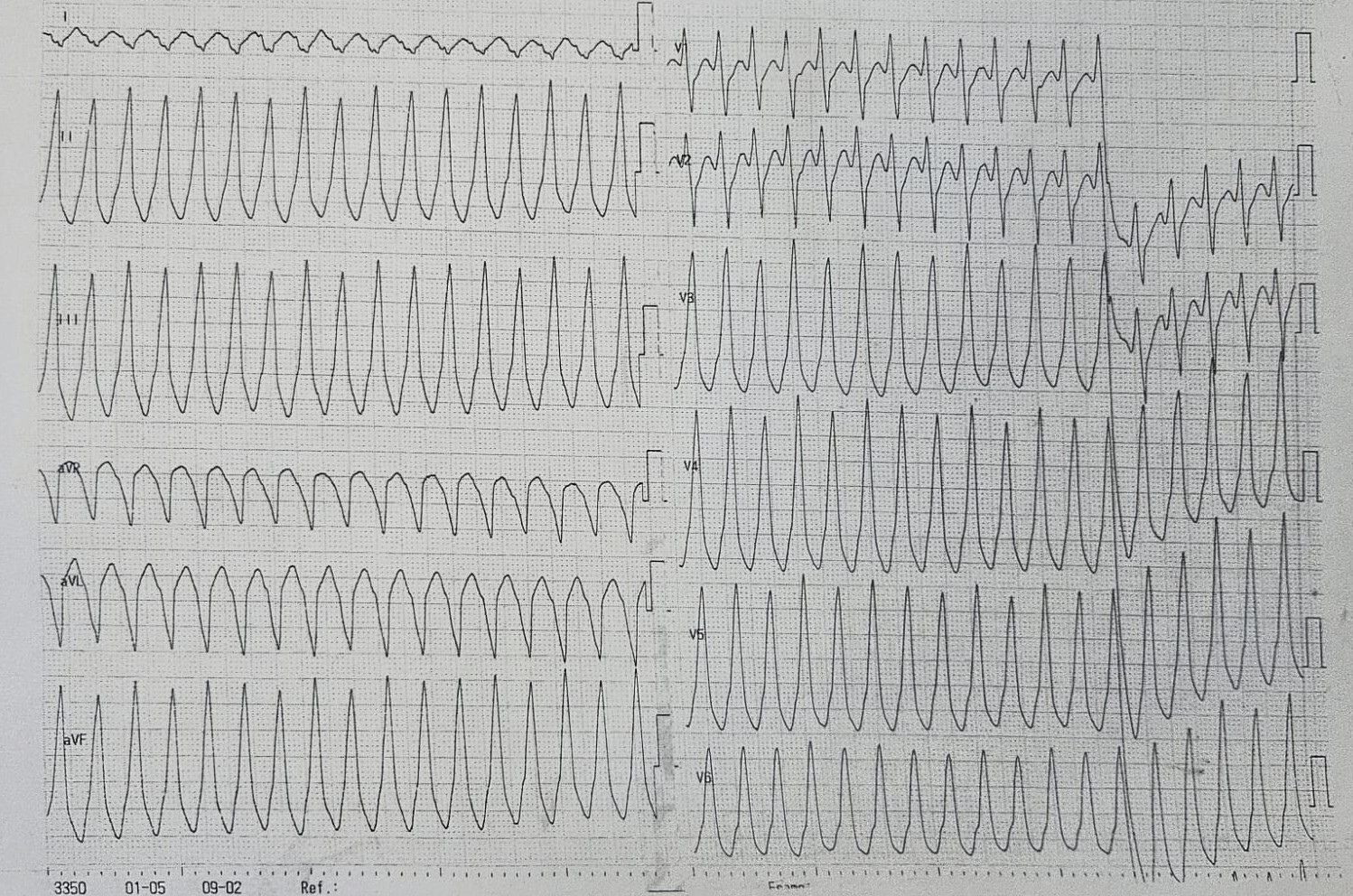
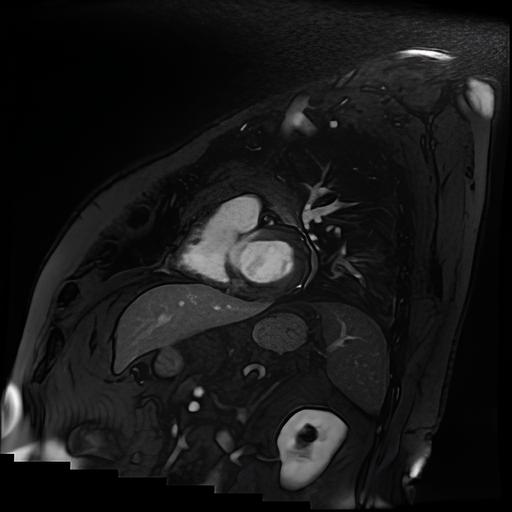
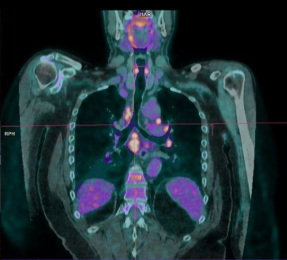
A 56-year-old man was admitted for palpitations and near-syncope. ECG documented sustained monomorphic ventricular tachycardia (VT), with QRS positivity in V3–V6 and inferior leads, suggesting a RVOT origin. Medical history included stage I pulmonary sarcoidosis treated with oral corticosteroids (OCS), stage II seminoma treated with left orchiectomy and chemotherapy in persistent remission, and a family history (FH) of sudden cardiac arrest attributed to non-investigated left ventricular (LV) cardiomyopathy (CM). Electrical cardioversion (ECV) restored sinus rhythm. Transthoracic echocardiography showed a normal-sized LV with diffuse hypokinesis, especially in the basal interventricular septum (IVS), and mildly reduced ejection fraction. HS-TnI peaked at 432 ng/L after ECV. Coronary angiography excluded obstructive coronary artery disease. Cardiac magnetic resonance (CMR) revealed hypertrophy of the IVS with preserved systolic function and no myocardial edema on T2-weighted imaging. Transmural LGE was noted in the basal IVS, along with increased T1/T2 mapping and extracellular volume values. 18F-FDG-PET demonstrated uptake limited to carinal lymph nodes, without evidence of active myocardial inflammation. According to the 2014 HRS consensus, a diagnosis of probable cardiac sarcoidosis (CS) was established based on histologically proven extracardiac sarcoidosis, sustained VT, and typical LGE findings. Alternative diagnoses, including arrhythmogenic CM, could not be fully excluded due to limited FH information. A dual-chamber ICD was implanted for secondary prevention. Given the absence of active inflammation on imaging, immunosuppressive therapy was initially withheld. A myocardial scar was identified as the arrhythmogenic focus, so amiodarone and heart failure (HF) therapy were initiated. At two-month follow-up (FUP), CMR-guided endomyocardial biopsy (EBM) was negative for granulomas, but its sensitivity is approximately 50%, thus not excluding CS. Device interrogation revealed an asymptomatic VT episode terminated by antitachycardia pacing, prompting beta-blocker up-titration. If VT requiring ICD discharges recurs nevertheless therapy, catheter-based RFA would be considered to reduce mortality and prevent HF progression. Despite lack of evidence of inflammation-triggered VT and a negative PET, low-dose OCS was increased to assess arrhythmic response and prevent further scarring. During 1-year FUP, no further VT occurred, so OCS were subsequently tapered