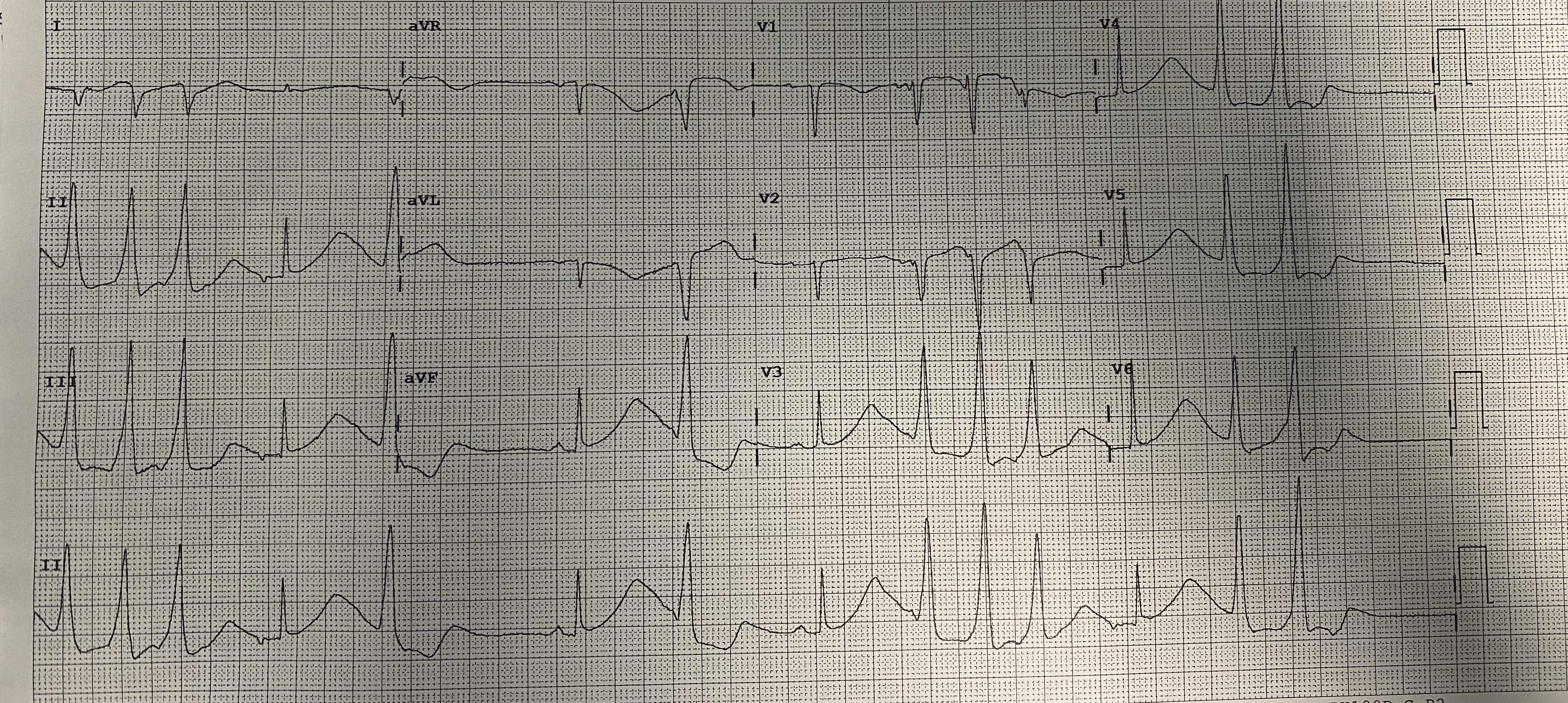
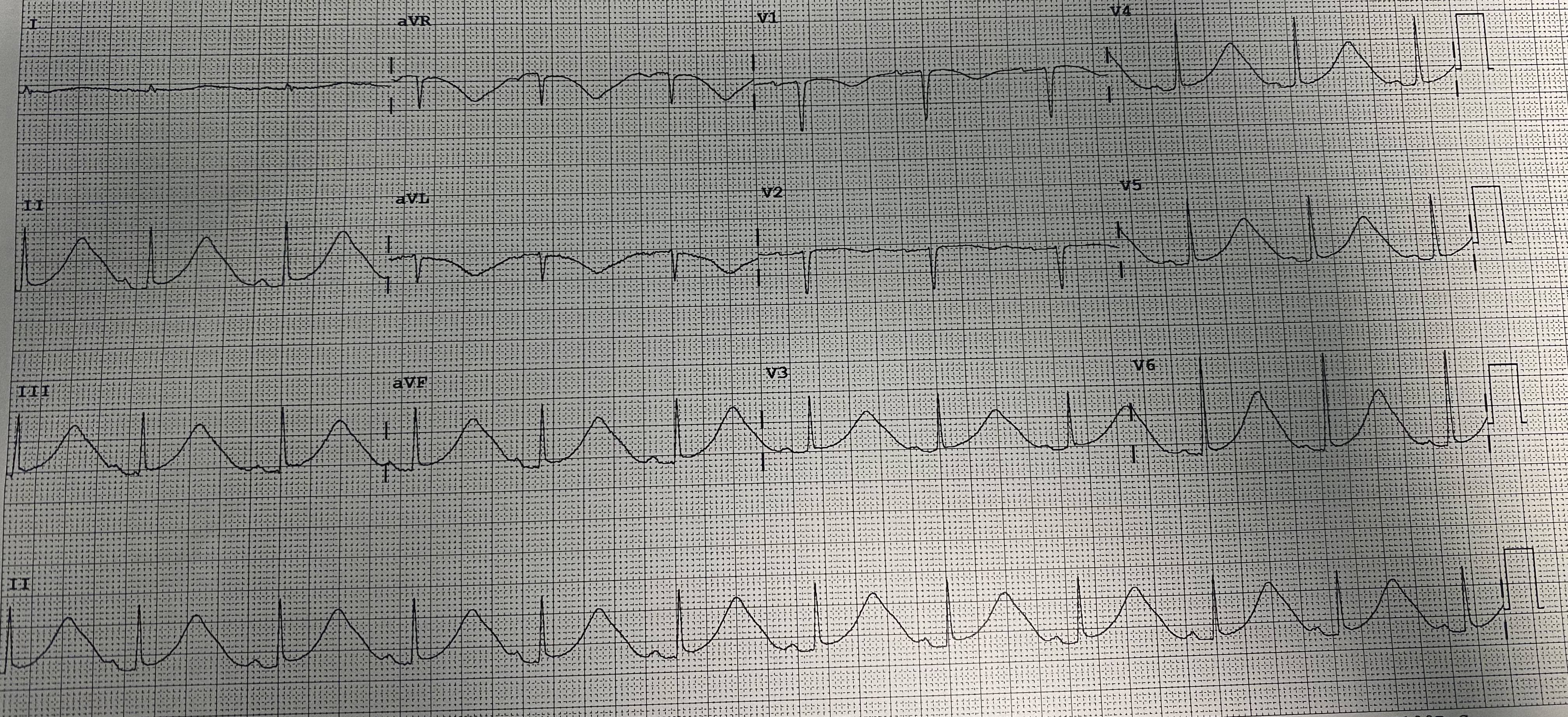
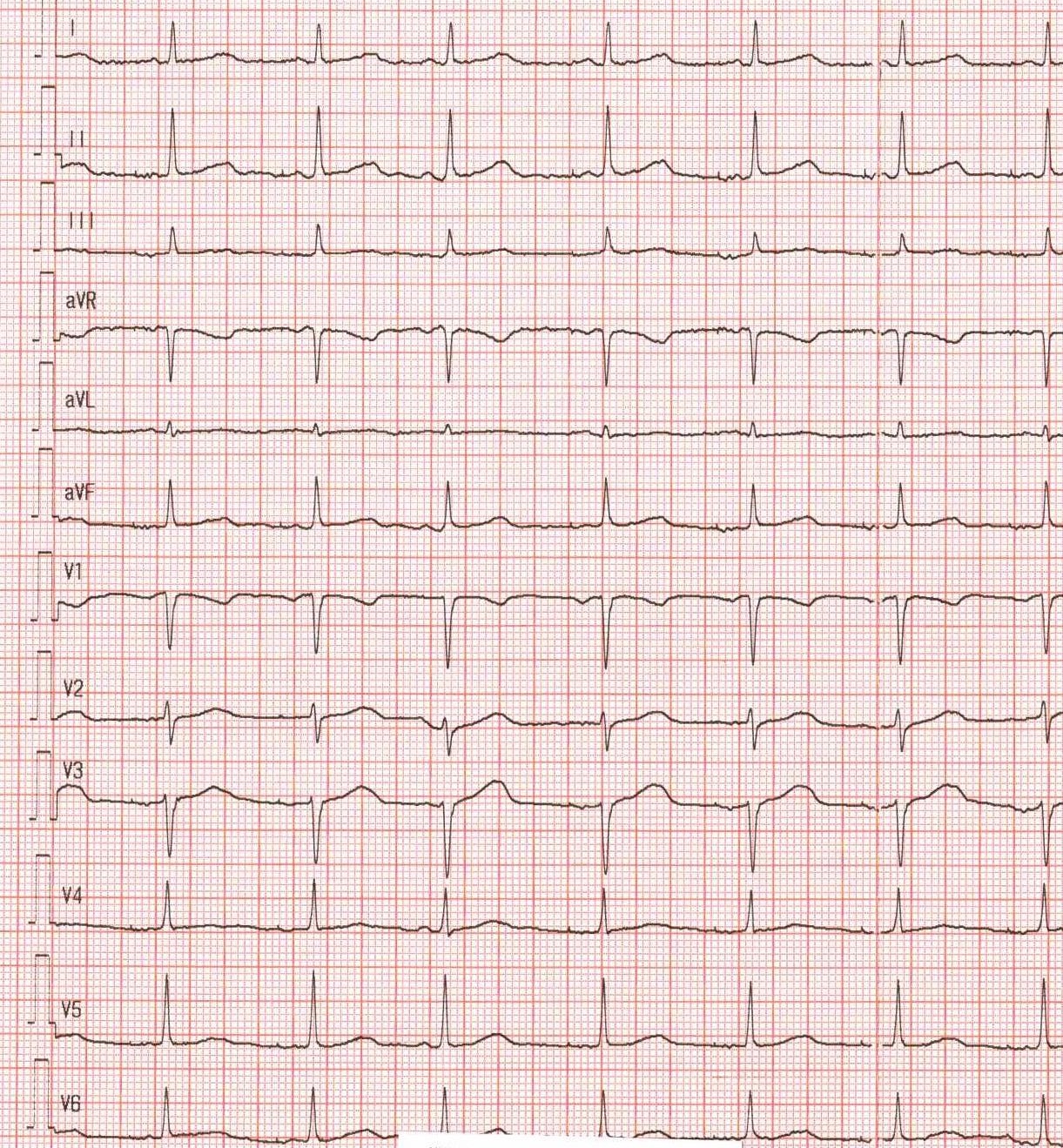
Long QT syndrome (LQTS) is a genetic channelopathy with a prevalence of approximately 1 in 2000. Type 2 (LQT2), caused by KCNH2 gene variants affecting the IKr current, is particularly prone to life-threatening arrhythmias triggered by sudden noises, emotional stress, or bradycardia. In the acute setting of an electrical storm, management remains a critical challenge. A 26-year-old female with a known KCNH2 mutation, already under treatment with Nadolol 80 mg daily, presented with an electrical storm. The patient had a concomitant diagnosis of epilepsy treated with Vimpat and Clobazam; therefore, an implantable loop recorder (ILR) had been previously inserted to evaluate a potential arrhythmic cause for her convulsive syncope. This device was fundamental in the diagnosis, as it documented multiple episodes of sustained ventricular tachycardia and a 2-minute episode of ventricular fibrillation, confirming the cardiac origin of her crises. At admission, the surface ECG showed a markedly prolonged QTc of 690 ms and notched T waves. Initial laboratory results showed a potassium level of 3.9 mmol/l. Acute stabilization was initiated with intensive electrolyte replacement and intravenous Esmolol. To address the electrical instability, a temporary external atrial pacemaker was programmed for overdrive pacing at 90 bpm. This strategy served as a crucial bridge to manage the acute phase, successfully suppressing Torsades de Pointes (TdP) and allowing for the safe re-introduction and up-titration of her Nadolol to 80 mg twice daily. The patient subsequently underwent successful implantation of a dual-chamber cardioverter-defibrillator (ICD). To prevent the bradycardia-induced pause-dependent prolongation of the QT interval typical of LQT2, the device was programmed with a base rate of 70 bpm. This higher heart rate prevents the long-short sequences that initiate TdP while allowing the patient to maintain the necessary high-dose beta-blockade. At discharge, the QTc had significantly shortened to 480 ms.