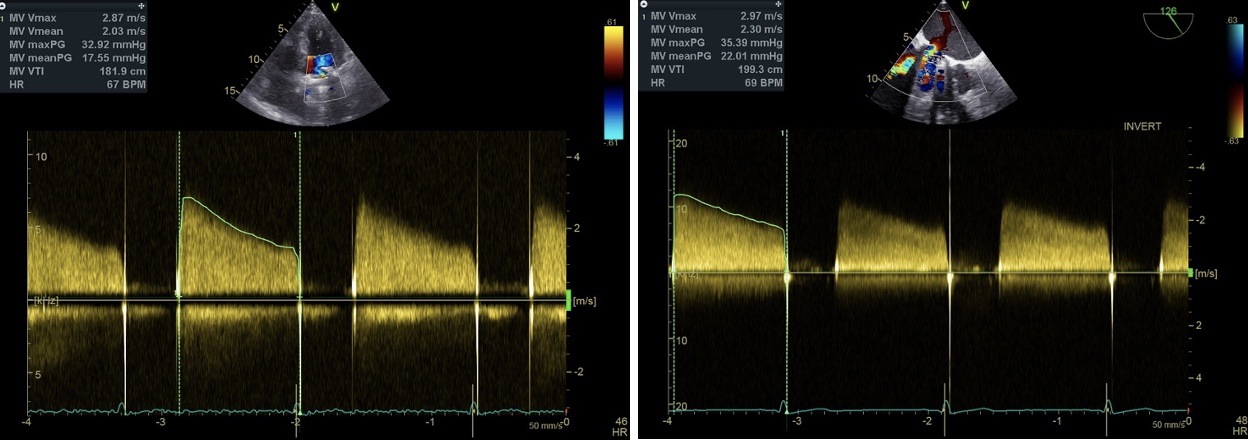
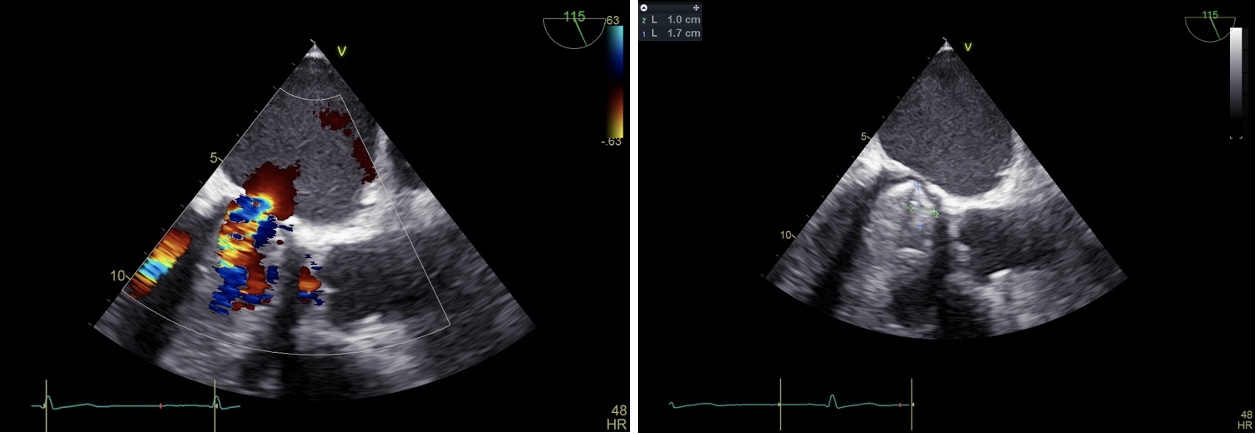
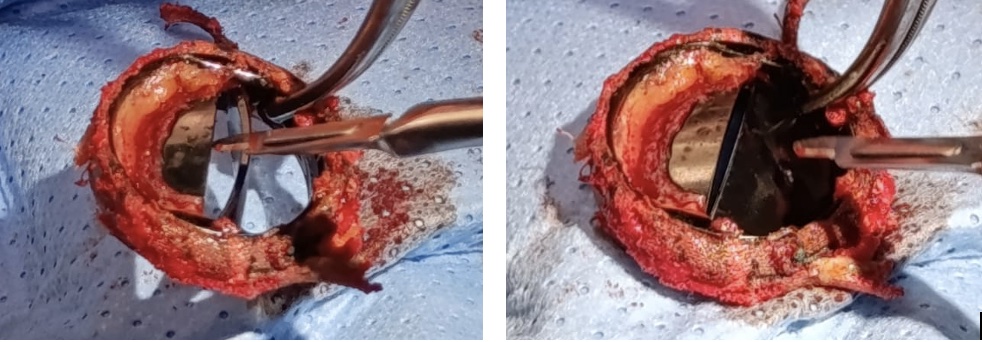
Introduction Mechanical valve (MV) dysfunction may result from thrombosis, pannus ingrowth, structural degeneration or infective endocarditis. Accurate identification of the underlying etiology is essential, as management differs substantially between thrombotic and non-thrombotic causes. The 2025 ESC guidelines on valvular heart disease emphasize multimodality imaging and Heart Team discussion for optimal decision-making in prosthetic valve dysfunction. Case Report A 60-year-old man with atrial fibrillation and combined mitro-tricuspid valve disease underwent mechanical mitral valve replacement with a Sorin Bicarbon 29-mm prosthesis, tricuspid annuloplasty and surgical AF ablation after progression from severe regurgitation to mitral stenosis. He presented with progressive exertional dyspnea and mild peripheral edema. Transthoracic echocardiography showed restricted prosthetic leaflet motion, elevated mean transprosthetic gradient (21 mmHg), and moderate-to-severe tricuspid regurgitation, raising suspicion of prosthetic valve dysfunction. Transesophageal echocardiography demonstrated reduced mobility of the antero-septal leaflet with a hyperechogenic structure consistent with obstruction. Contrast-enhanced chest computed tomography excluded prosthetic valve thrombosis. Given persistent symptoms and imaging findings, the case was discussed by the Heart Team. Surgical exploration revealed fibrous pannus and annular calcification limiting leaflet mobility. The mechanical prosthesis was replaced with a 29-mm Medtronic Hancock bioprosthesis, and tricuspid repair was revised. Postoperative recovery was uneventful, with normalization of transprosthetic gradients and improvement in functional status. Discussion Differentiating thrombus from pannus is crucial, as thrombotic obstruction may respond to anticoagulation or thrombolysis, whereas pannus requires surgical treatment. Chronic symptom progression, adequate anticoagulation, hyperechogenic and immobile lesions, and absence of thrombus on CT support the diagnosis of pannus. Current guidelines recommend multimodality imaging and Heart Team evaluation to guide personalized therapy. Conclusion This case illustrates the challenges in diagnosing mechanical prosthetic valve dysfunction. Accurate etiological differentiation through imaging and multidisciplinary discussion is essential to optimize patient management and outcomes.