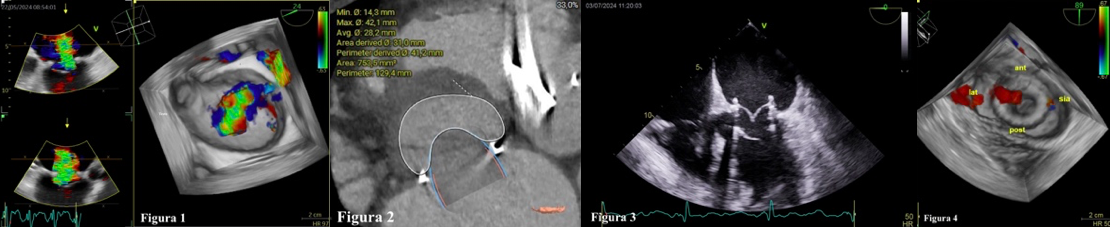
CLINICAL CASE: 69-year-old woman underwent myectomy according to Morrow and mitral anuloplasty by complete CE Physio II ring No. 34 in 2015 for severe functional mitral regurgitation; subsequent gradual worsening of left ventricular systolic function and reappearance of mitral regurgitation treated with CRT-D implant, not followed by recovery of left ventricular FE. In subsequent years repeated admissions for heart failure associated with worsening mitral insufficiency. Last admission in June 2024 for congestive heart failure in the course of ventricular tachycardia and atrial fibrillation treated with atrio-ventricular node ablation. During the hospital stay, after stabilisation of the rhythm and haemodynamic picture by means of vasodilators and inotropes, the transthoracic echocardiogram (ETT) showed: reduced left ventricular systolic function (FE 30%), severe mitral insufficiency as a result of mitral anuloplasty with central jet from bilembus tethering and moderate-severe tricuspid insufficiency with elevated pulmonary pressures. Subsequent transesophageal echocardiogram (ETE) confirmed the severity of functional mitral regurgitation (EROA 3D 0.7 cmq, VC 2D 8 mm) in the presence of extensive flap tethering, prevailing for the posterior flap, smaller para-annular jet, at A2, from probable tear (VC 2D 3 mm) (fig.1). After collegial discussion, in view of the echocardiographic findings, the aortic angio-CT with study of the neo-LVOT (Fig. 2), the clinical symptoms, the frequent flare-ups of congestive heart failure, and the high cardiac surgical risk (Euroscore 23.64 %), the indication was given for a percutaneous attempt to implant an Edwards Sapiens Ultra 29 mm valve prosthesis using the Valve-in-Ring technique. At the post-procedural ETE, the mitral valve prosthesis was well positioned (fig.3) with no LVOT obstruction and well functioning (mean G 2 mmHg, PHT area 3.6 cmq) with minimal medial peri-prosthetic leak, minimal intra-prosthetic regurgitation (fig.4) and modest residual sn-dx shunt at transseptal puncture. DISCUSSION: Recurrence of major mitral regurgitation in previous mitral ring anuloplasty occurs in up to 30 % of patients 10 years after the procedure. Although reoperation is the gold-standard of treatment, it carries a high operative risk. An alternative is percutaneous implantation of a biological prosthesis by means of a valve-in-ring technique, also using prostheses designed for percutaneous aortic valve replacement with good results.