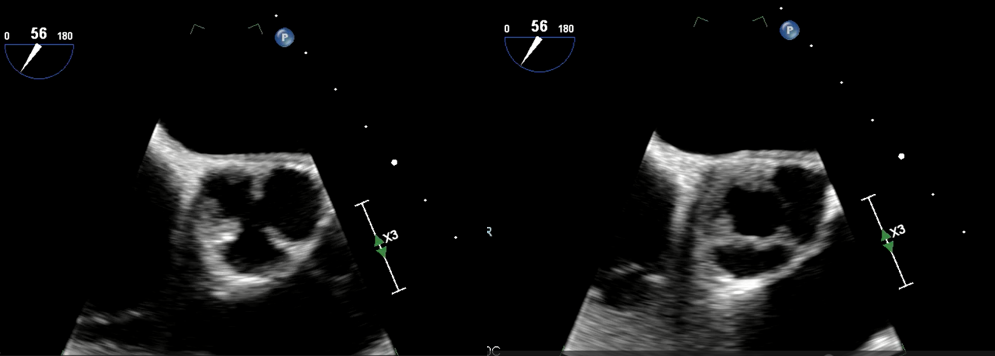
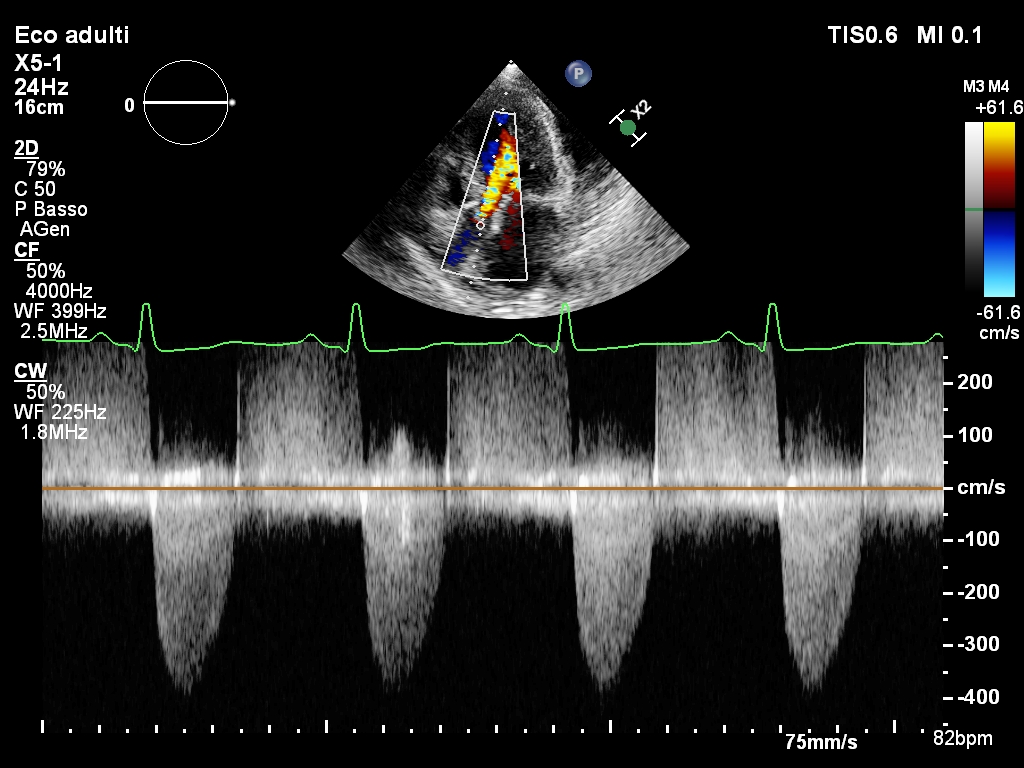
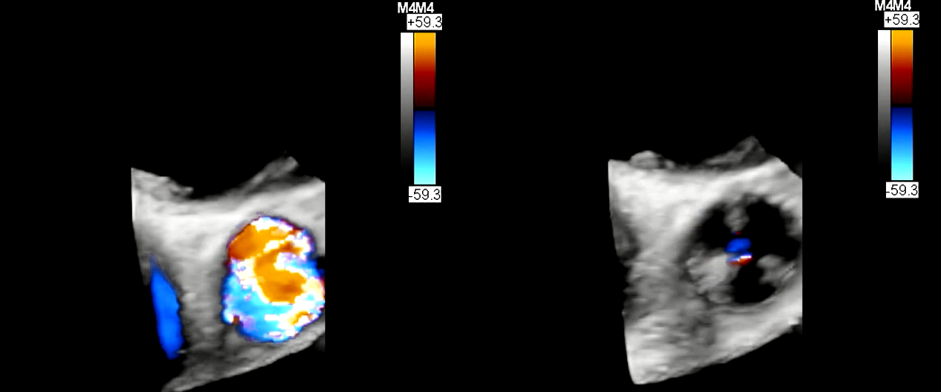
Introduction Aortic valve stenosis (AS) is a leading form of cardiovascular disease in the developed world, affecting 0.3 – 0.5 % of the general population.The etiologies of AS are different, the most frequent is the degenerative form in elderly population,followed by congenital malformation (unicuspid or bicuspid aortic valve) and rheumatic heart disease (RHD) especially in young population.Echocardiographic exam allows to assess early stage of disease before the onset of symptoms and to orientate the adequate timing of aortic-valve replacement.Case Report A 53 years old female admitted to our medical centre with history of dyspnea for mild exercise and chest pain. On his physical examination body temperature was 37,4 °C, blood pressure was 100/60 mmHg,and heart rate 100 beats/min.ECG showed sinus rhythm, high voltage QRS and no changes of ST-T waves suggestive for ischemia.On admission,hematologic findings, renal and liver function tests were within normal limits.C-reactive protein was slightly increased.Myocardionecrosis enzymes were elevated.Echocardiographic examination documents reduced ejection fraction(EF 45%)with diffuse hypokinesia, severe aortic valve stenosis and moderate aortic insufficiency and pericardial effusion.Diuretic supportive therapy was first initiated.On the suspicion of peri-myocarditis was treated whit antiinflammatory drugs.All autoimmune tests were negative.To better evaluated aortic valve disease a transoesophageal echocardiogram was perfomed hat showed leaflet thickening and calcification with circular valve opening. The peak and mean aortic valve gradients were recorded to be 66 mmHg and 42 mmHg, respectively.The valve area calculated by planimetry was 0.874 cmq in 2D. Calculated valve area by continuity equation was 0.562 cm2/m2.A unicuspid aortic valve was suspected.Coronary angiography was negative for stenosis.A cardiac magnetic resonance imaging was performed and no diagnostic criteria for myocardial inflammation was detected.After stabilizing the clinical condition, the patient underwent surgical replacement of the aortic valve. A diagnosis of rheumatic aortic valve disease was made because the valve was tricuspid and had fusion of the cusps.ConclusionRHD and congenital aortic valve malformation have a different prevalence in the general population. Today there are many tools available for a reliable diagnosis.Cardiac MRI, thanks to better image quality, can help in the diagnosis and specific treatment for our patient