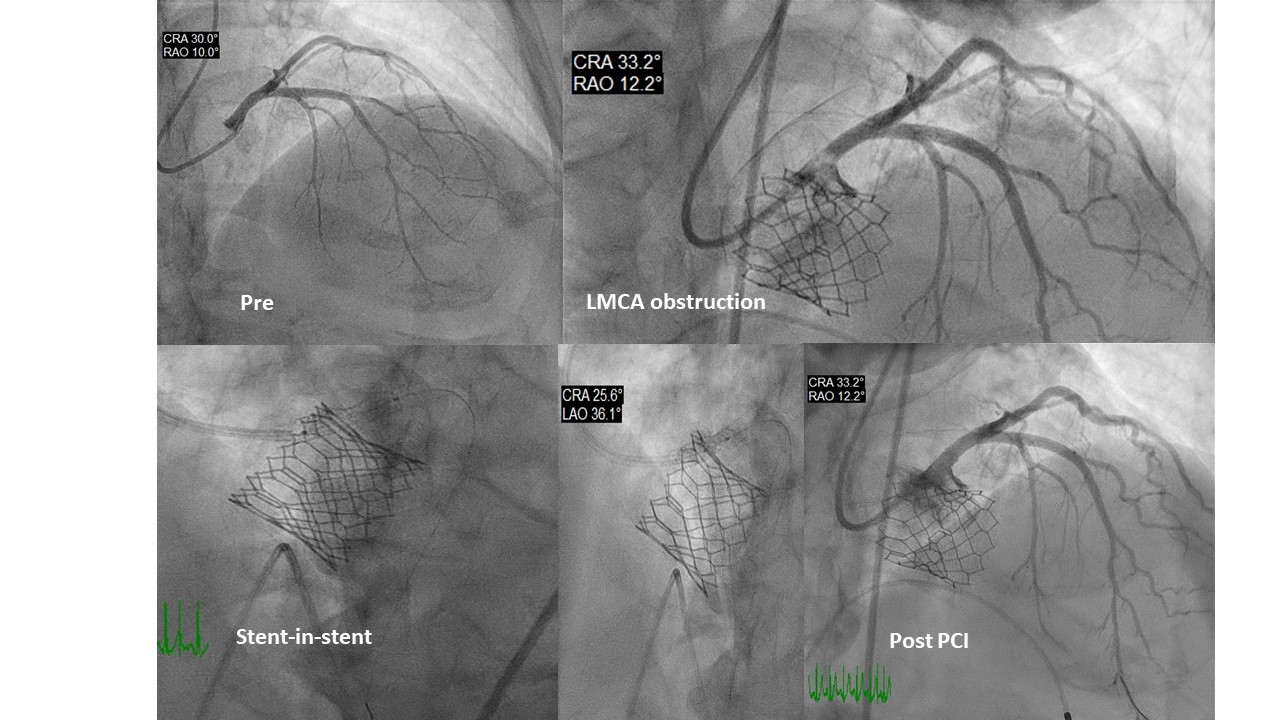
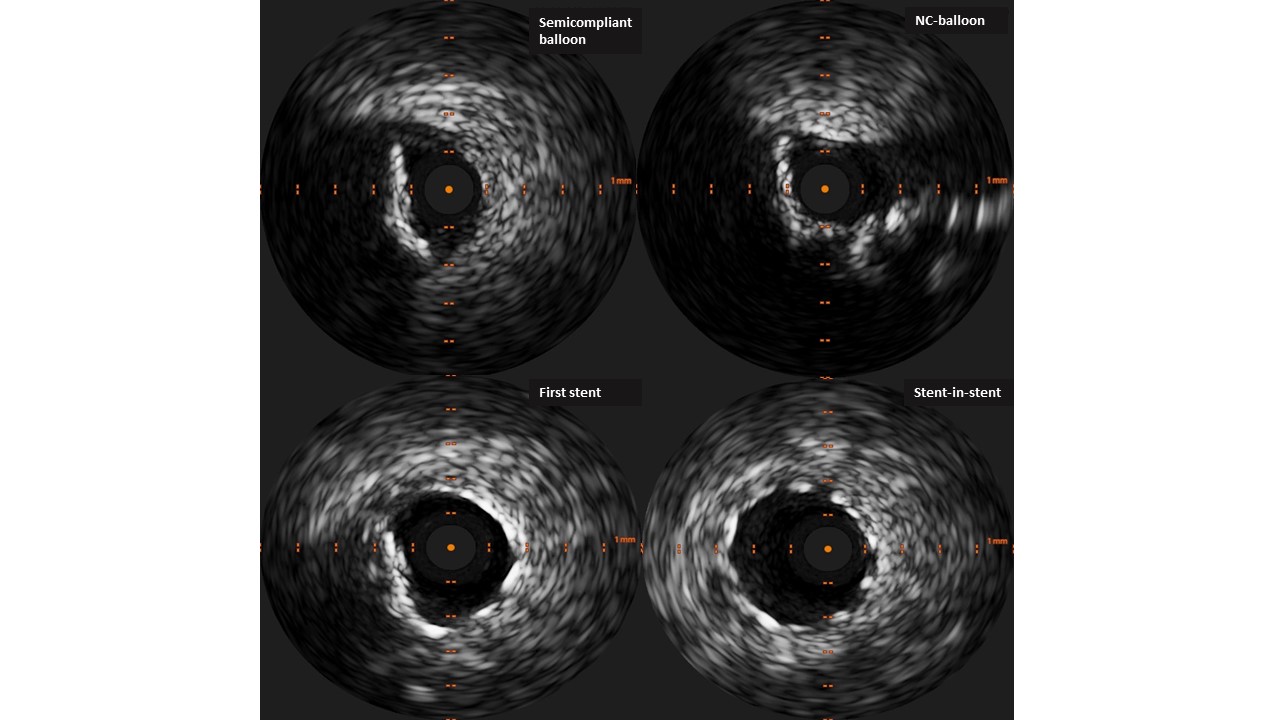
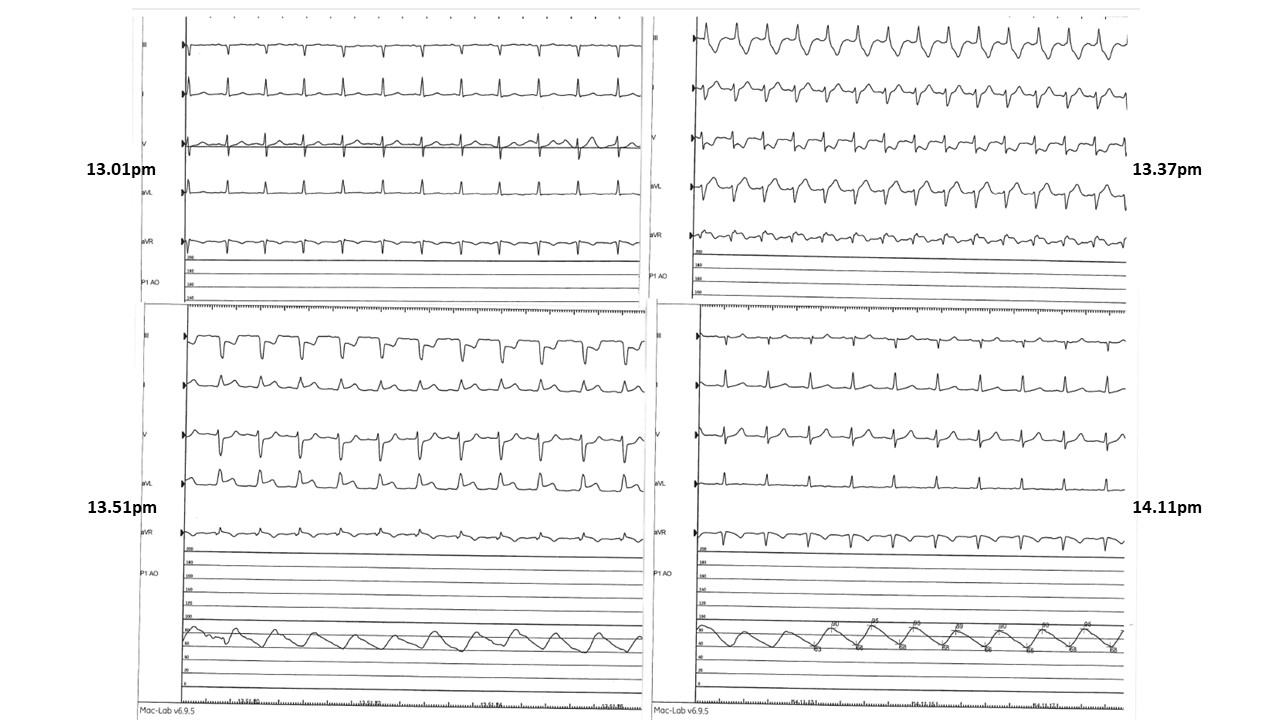
Background: The occurrence of left bundle branch block (LBBB) during transcutaneous aortic valve implantation (TAVI) has an incidence of 5 to 65% and is due to mechanical damage to the conduction system, while the right bundle branch block (RBBB) or left posterior hemiblock (LPH) are very rare and associated with myocardial ischemia. The right bundle branch receives its blood supply from anterior descending coronary artery. Acute left main coronary artery (LMCA) occlusion during TAVI is a life-threatening complication, with an incidence of 0.6% but a 30-day mortality rate of up to 50%. The most likely mechanism is the obstruction by the native aortic valve (AV) leaflet. However, acute LMCA occlusion due to calcific plaque shifting has been rarely reported. Case presentation. A 71-year-old woman presented to our department with acute heart failure. Electrocardiography (ECG) showed sinus rhythm; transthoracic echocardiogram (TTE) revealed severe AV stenosis (AV area 0.62 cm2) and left ventricular ejection fraction (LVEF) of 46%. Coronary angiogram was normal. Computed tomography showed an aortic annulus size of 26/20 mm, sinus of Valsalva size of 33 mm, annulus area of 442 mm2, heavily calcified leaflets, height of LMCA 11 mm, and right coronary artery of 12 mm. Despite an intermediate-risk (STS-PROM 5%, EuroSCORE II 9.1%), the informed patient insisted on a TAVI treatment. The procedure was performed under deep sedation with the implantation of a 26 mm balloon-expandable valve, with good results. For the immediate appearance of RBBB/LPH and subsequent evidence of diffuse ST segment depression on the ECG, an angiogram was performed with evidence of obstruction of the LMCA (Fig. 1). Percutaneous coronary intervention (PCI) to the LMCA was performed with one drug-eluting stent. Intravascular ultrasound (IVUS) demonstrated underexpansion of the stent, which was not responsive to high-pressure non-compliant balloon dilatation. Therefore, we deployed a stent-in-stent, with better expansion (Fig. 2). Following PCI, the ECG immediately returned to normal, with RBBB/LPH disappearing (Fig. 3).The patient was discharged on Day 3. At 6 weeks follow-up, TTE demonstrated normal LVEF and AV function. Conclusions. Acute LMCA occlusion is a rare life-threatening complication of TAVI that is poorly predictable and requires immediate diagnosis/treatment. RBBB/LPH is an ominous sign, and the good old “ECG” with knowledges of anatomy/physiology can save the patient's life.