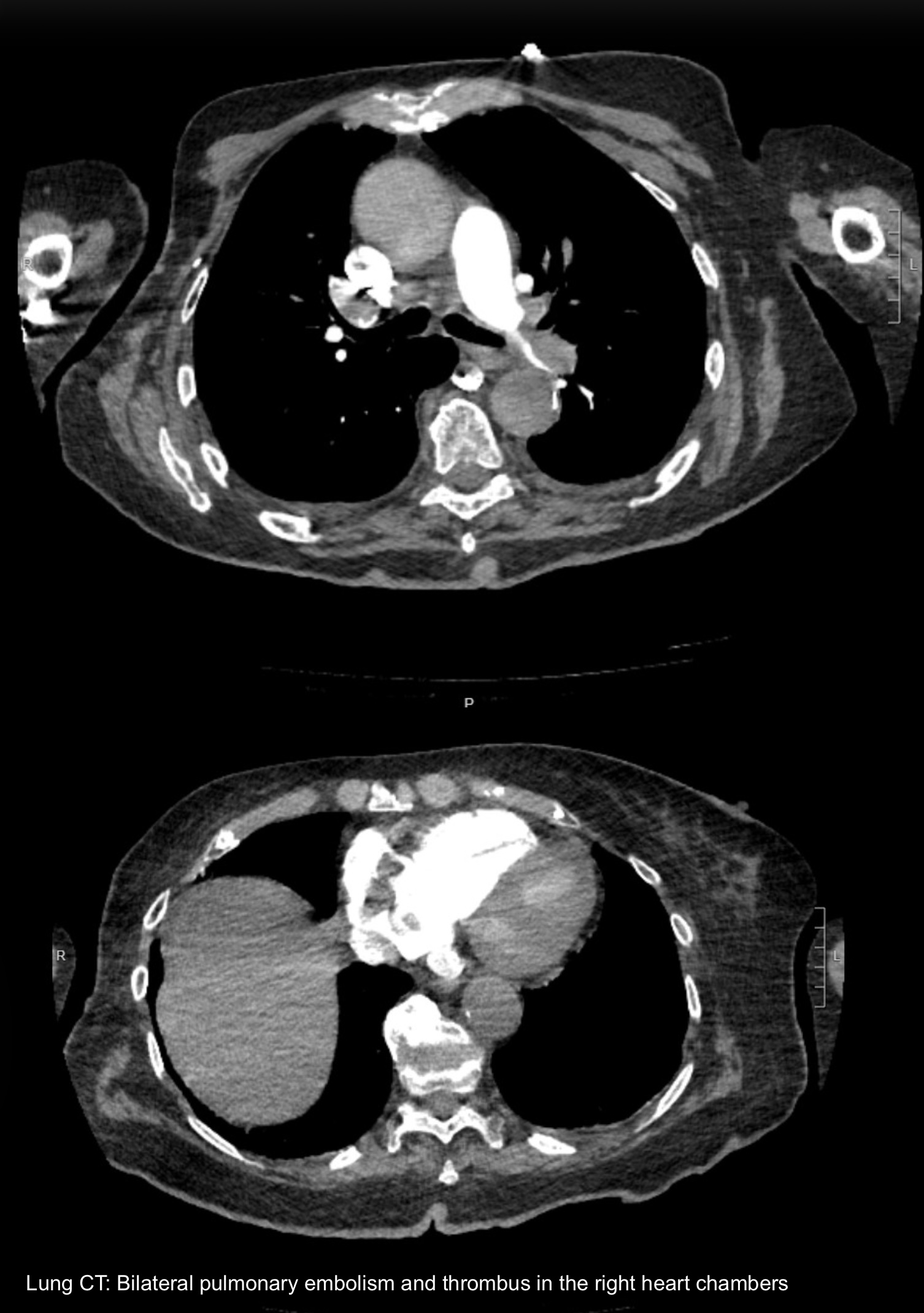
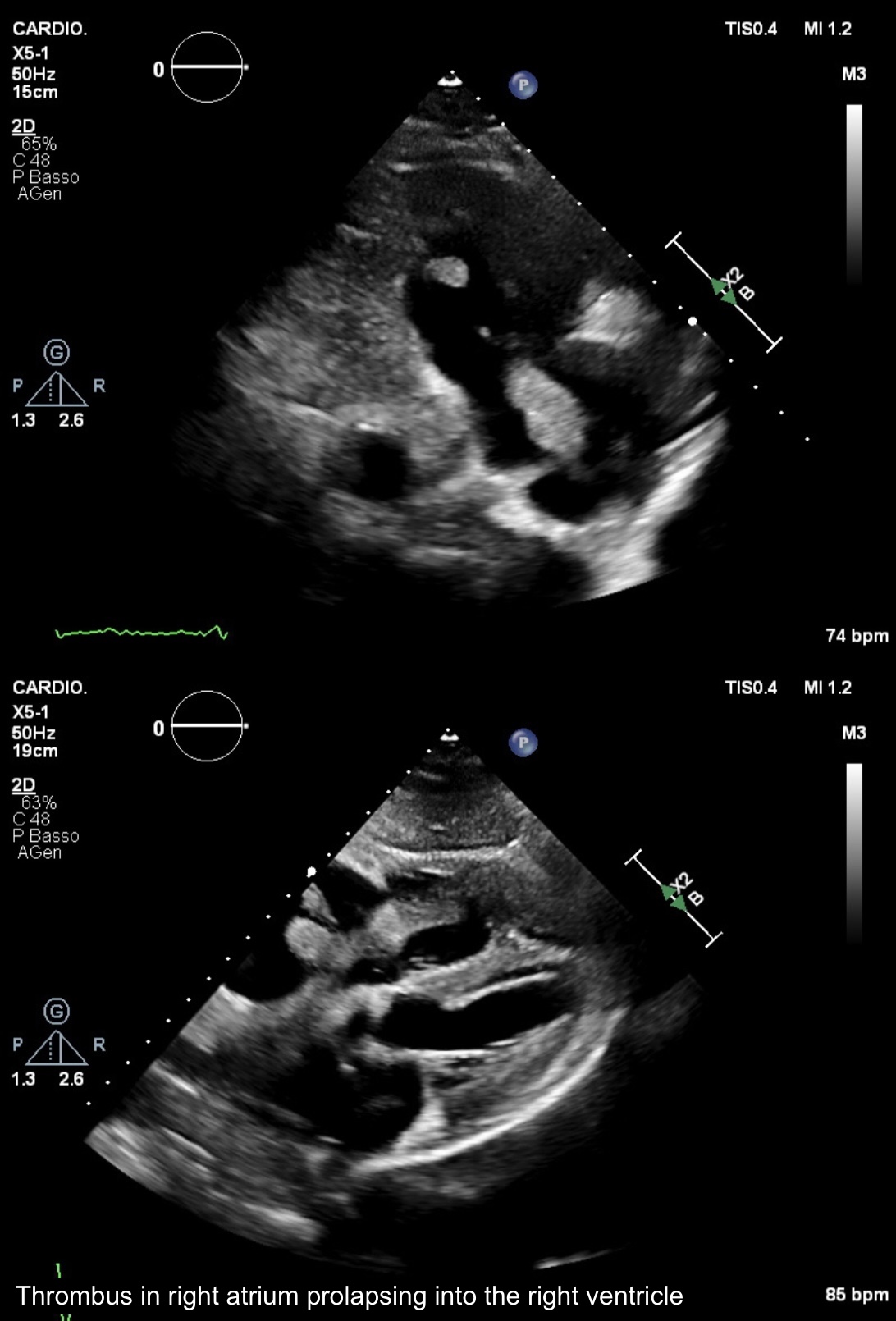
Introduction : Massive pulmonary embolism is associated with high mortality and requires immediate treatment. Mechanical thrombectomy is an effective therapeutic option for patients at high hemodynamic risk who have contraindications to systemic thrombolysis. Case report : An 82-year-old woman with a history of hypertension, dyslipidemia, permanent atrial fibrillation, and breast cancer presented to the emergency department with acute dyspnea, chest pain and hypotension. Arterial blood gas showed severe hypoxemia, hypocapnia and hyperlactatemia. The patient had recently undergone total left knee replacement, with temporary discontinuation of NOAC therapy and initiation of LMWH 4,000 IU once daily. The ECG showed a new-onset right bundle branch block. Blood tests revealed a markedly elevated D-dimer (10,672 ng/mL) and elevated high-sensitivity troponin. A lung CT scan performed for suspected pulmonary embolism demonstrated extensive bilateral pulmonary thromboembolism involving lobar and segmental branches and a large right atrial thrombus. The echocardiogram confirmed the presence of a mobile thrombus (10 cm × 16 mm) in right atrium prolapsing into the right ventricle, acute right ventricular overload signs, dilated inferior vena cava and severe pulmonary hypertension (sPAP 50 mmHg). Due to the high PESI/sPESI risk scores and deterioration of hemodynamic status, intravenous heparin and inotropic support were initiated. Considering the recent major orthopedic surgery and the associated high bleeding risk, mechanical thrombectomy was selected as the treatment strategy. The procedure was performed under echocardiographic and angiographic guidance, achieving complete thrombus removal and pulmonary reperfusion. Post-procedural echocardiography demonstrated normalization of right ventricular function, absence of residual thrombi, and hemodynamic stabilization. Lower extremity venous Doppler revealed bilateral deep vein thrombosis showing signs of recanalization. Elastic stocking therapy was initiated, with concomitant initiation of NOAC therapy and close clinical follow-up. Conclusions : This case highlights the importance of early recognition of thromboembolic complications in unstable postoperative patients and the role of mechanical thrombectomy as an effective alternative to systemic thrombolysis.